Эта статья опубликована под лицензией Creative Commons и не автором статьи. Поэтому если вы найдете какие-либо неточности, вы можете исправить их, обновив статью.

Whole-body vibration and benefits for people with osteoarthritis: A systematic review



Pedro Ronikeile da Costa
Danúbia da Cunha Sá-Caputo
Adriano Arnóbio
Dulciane Nunes Paiva
Rafaelle Pacheco
Cristiane Kutter
Rebeca Costa
Paula Mantilla Giehl
Pedro Jesus Marin
Jay R. Salmon
Mark Tillman
Mario Bernardo-Filho
Опубликована Сен. 30, 2014
Последнее обновление статьи Авг. 19, 2022
Эта статья опубликована под лицензией
")



Abstract
Whole body vibration (WBV) can be an important tool to treat patients with osteoarthritis (OA). The purpose of this study was to systematically review published research concerning the use of WBV in people with OA. In PubMed and Scopus, the number of publications (NP) is respectively to the keywords arthrosis, 289,586 and 10,569, osteoarthrosis, 299,158 and 3,952, arthritis, 251,453 and 236,849 and osteoarthritis, 56,323 and 80,008. Putting together the information found in the analyzed 4 papers, the numbers of subjects were ranging from 15 to 52 and frequencies ranging from 24 to 40 Hz. Self-report of the status of disease (WOMAC) was used in 2 papers, while the pain levels were evaluated by the visual analog scale (VAS) in 2 papers. Different tests were used in these studies, as (i) TUG, (ii) step test, (iii) 20-meter walk test, (iv) timed get up and go test (TGUG), (v) chair stand test (CST), (vi) 6-minute walk test (6MWT), (vii) knee muscle strength (extension/flexion) and (viii) proprioception (threshold for detection of passive movement (TDPM) to evaluate the effects promoted by the exercises due to the WBV. In conclusion, these studies indicate that the WBV could bring some benefits to patients with OA.
Ключевые слова
Osteoarthrosis, Scopus, oscillating/vibratory platform., arthritis, whole body vibration, arthrosis, PubMed
INTRODUCTION
Joints are functional units of the body that aid in the transmission of mechanical loads between contacting the bones during normal daily activities or in special situations related with sports and work. All the components of the joint, including the articular cartilages (AC), bone, muscles, ligaments/tendons, nerves and synovial fluid participate in load transmission (Arokoski et al., 2000; van den Berg, 2010).
AC are found on the epiphyses of long bones and function to cushion, to act as load-bearing structures and, in consequence, to reduce the friction in the articular sur-faces. AC composed of a smooth, lubricated, reversibly compressible tissue that protects the underlying bones from biomechanical damage during joint loading. Failure in one or more of the components of the joint can cause joint malfunction, which, in turn, may lead to the accumulation of damage in other joint components and impairment of the entire body (Eyre et al., 2006; Wu et al., 2011).
Articular cartilages and ostheoarthritis
AC have received much of the attention in osteoarthritis (OA) studies, because gross AC damage is the most obvious pathologic feature leading to joint dysfunction. Miehle (1987) has reported that in contrast to German-speaking regions, where the expression "arthrosis" is used, English-speaking countries prefer the term "osteoarthritis" to express disorders of the articular cartilage. Arthritis, arthrosis, osteoarthritis and osteoarthrosis are other terms used in the investigations of the clinical disorders associated with the AC (Lievense et al., 2002).
Patients diagnosed with AC defects are at increased risk for the early development of OA (Gillogly et al., 1998; Charlton et al., 2008). OA is the most common form of arthritis in the USA (Lawrence et al., 2008; Loeser, 2006; National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), 2013), and the most prevalent and degenerative joint disorder worldwide (Reginster, 2002; Stein et al., 2010). In addition to being the most prevalent form of arthritis, knee pain associated with OA is the leading cause of disability in older adults (Peat et al., 2001). The central feature of OA is the destruction and loss of the AC of the articulating bones, which can lead to the dysfunction of the joint (Loeser, 2006; NIAMS, 2013). Moreover, AC degenerates with the development of fibrillation and fissures, and full thickness loss of the joint surface (French et al., 2013). In contrast to other forms of arthritis, such as rheumatoid arthritis, a systemic disorder of the immune system that can affect the skin, lungs, eyes, and blood vessels, OA affects only the function of the affected joint (NIAMS, 2013).
Mechanical forces have strong influence on the synthesis and rate of turnover of AC molecules, such as proteoglycans (PG). Moreover, regular cyclic loading of the joint, (i) enhances the synthesis of PG, increasing the rigidity of the cartilage and (ii) appears to have fewer effects on the AC collagen fibril network. Continuous compression of the AC diminishes PG synthesis and can cause injuries of the tissue due to possible necrosis. Moreover, it is suggested that OA starts from the cartilage surface due to the PG depletion and fibrillation of the superficial collagen. Several investigations have been published about alterations of structures neighboring the joint and related to abnormalities in the gross appearance, material properties, cellular morphologies, biochemical composition, and gene expression in AC in human beings and in animals with AO (Loeser, 2006; Goldring and Goldring, 2007; Meulenbelt et al., 2007; Bijlsma et al., 2010; van den Berg, 2010; Schroeppel et al., 2011; Wang et al., 2011). Characteristics of OA include (i) phenotypic changes in the cells of the super?cial layer of the AC, (ii) chondrocyte hypertrophy and apoptosis, (iii) progressive fibrillation and fissures of the AC, (iv) subchondral bone sclerosis, (v) bony outgrowths (osteophyte) formation, and (vi) increased remodeling of the periarticular bone (French et al., 2013; Bijlsma et al., 2010; van den Berg, 2010).
Ostheoarthritis and treatments
AC have received much of the attention in OA studies because gross AC damage is the most evident pathologic characteristics leading to joint dysfunction. There are no proven treatments capable of markedly altering the progression of the OA (The American College of Rheumatology (ACR), 2013; Osteoarthritis Research Society International (OARSI), 2013). Zhang et al. (2008) have reported evidence-based guidelines for the medical management of knee OA based upon systematic reviews of previously published guidelines, meta-analyses, reviews, and studies. Moreover, the ACR and OARSI state the goals of treatment of knee OA as (a) reducing joint pain and stiffness, (b) improving joint function and reducing disability, (c) improving health-related quality of life, (d) limiting the progression of joint damage and (e) avoiding any toxic effects of therapy, if possible.
ACR (2013) and ORSI (2013) agree that the preferred treatment of knee OA would involve a combination of pharmacologic and nonpharmacologic therapies, with pharmacologic therapies added to the nonpharmacologic modalities as indicated by individual circumstances.
Nonpharmacologic modalities of treatment
Exercise appears to be the most recommended nonpharmacologic treatment for knee OA. ACR and OARSI suggest aerobic exercise and resistance training (to strengthen periarticular muscles such as the quadriceps) as treatments that have been shown to modestly, yet significantly, improve the range of motion (ROM) of the knee, reduce pain, improve function and reduce disability.
Additional benefits of exercise programs mentioned in the ACR guidelines include less analgesic consumption, fewer visits to a physician, improved knee joint position sense, and improved performance of activities of daily living lasting up to six months.
Additional nonpharmacologic treatments recommended by the ACR and OARSI include walking aids such as walkers, canes, or crutches used in the contralateral hand. These aids can reduce loading in the affected knee leading to reduced pain and improved physical functioning. Further recommendations include wedged insoles, medial patella taping, and knee braces to correct abnormal biomechanics contributing to OA symptoms. These modalities have been shown to reduce pain, instability, and risk of falling. Heat therapy and cryot-herapy, acupuncture, and transcutaneous electrical nerve stimulation are additional therapies recommended, to a lesser degree, by the OARSI for the management of knee OA symptoms.
Pharmacologic modalities of treatment
Because of its safety and efficacy, the simple analgesic acetaminophen is recommended as the preferred pharmacologic treatment for mild to moderate knee OA pain, especially for long-term use. Evidence presented by the ACR shows some disagreement regarding the efficacy of acetaminophen as compared to nonsteroidal antiinflammatory drugs (NSAIDs). While some studies indicate that acetaminophen is as effective as NSAIDs in relieving mild to moderate joint pain, other studies suggest a greater improvement in pain with NSAIDs. Yet additional studies suggest that they may be equally effective in relieving mild to moderate joint pain, with NSAIDs being more effective in treating severe pain.
In patients not effectively responding to oral analgesics, treatments involving injections directly into the joint such as glucocorticoids and hyaluronic acid (HA) are recom-mended, to a lesser degree, by both groups. For patients whom have not responded to other pharmacologic treatments or in cases where other treatments are contraindicated, both groups recommend the use of weak opioids (e.g. tramadol, codeine) and narcotic analgesics for the relief of moderate to severe knee OA pain. Stronger opioids (e.g. oxycodone, fentanyl, morphine) should be reserved for the treatment of severe pain in extreme circumstances. The negative influence of such side effects on fall risk and quality of life in the knee OA pa-tient underscore the limitations of opioids as a treatment (Goodwin et al., 2005; ACR, 2013; OARSI, 2013).
Glucosamine and chondroitin sulphate, two naturally occurring components of cartilage proteoglycans, are often taken as nutritional supplements by individuals with OA. They are recommended, to some degree, by the OARSI for the treatment of knee OA, although mixed evidence exists regarding efficacy in pain reduction and functional improvement. Small amount of evidence is presented by the OARSI suggesting that they may have beneficial structure-modifying effects in the knee joint.
Surgical interventions
When a combination of nonpharmacologic and pharma-cologic treatments fails to provide adequate pain relief and functional improvement in severe knee OA cases, there are a number of surgical procedures recommended by the ACR and OARSI. Total joint arthroplasties are recommended by both groups with evidence indicating reduced pain, improved function, and improved health-related quality of life in many cases. Osteotomy is recommended by both groups as a means of correcting abnormal biomechanics in the knee, and slowing the progression of OA. Finally, arthroscopic debridement to remove debris such as loose cartilage and meniscus fragments is recommended by both groups, but less strongly. In spite of the evidence in favor of their effectiveness in treating severe cases of knee OA, the combination of the financial costs, and the psychological and physical health risks associated with surgery (Lingard and Riddle, 2007; Patella et al., 2008; Webb et al., 2008; Haas et al., 2008), especially in a population characterized by advanced age and frequent comorbidities, make surgical treatment of knee OA undesirable in many cases, and unfeasible in others. An alternative treatment, such as, whole body vibration (WBV) could prove beneficial.
Whole body vibration and the oscillating/ vibratory platform
Vibration is a mechanical stimulus that is created by an oscillating/vibratory motion that it usually delivered through an oscillating/vibratory platform. Vibration can be characterized by its magnitude and its frequency. The magnitude is determined by the amplitude, or peak to peak displacement of the oscillation. The frequency is measured in oscillations per second. Together, these factors determine the intensity of the vibration (Rittweger, 2010).
Vibration has long been studied for its negative effects on the body, usually as the result of exposure in the workplace to either high intensity vibration or chronic exposure to large amounts of vibration over many years. These negative effects have been summarized in pre-vious reviews and include damage to nerves, blood vessels, and joints (including the spine), as well as disruption of proprioception, vision, and hearing (Jordan et al., 2005; Lings and Leboeuf-Yde, 2000; Seidel, 1993; Abercromby et al., 2007). In spite of the existing negative reports, much research has been conducted regarding the potential beneficial effects of the WBV on the body.
Cardinale and Wakeling (2005) emphasize that vibration is a natural stimulus that we experience every-day as our bodies are acted upon by external forces, while interacting with our environment. They note that vibrations are commonly experienced in sporting activities and that the transmission of these vibrations throughout the body is dependent upon the properties of numerous different tissues including bone, cartilage, and muscle. Previous reviews provide evidence of the numerous effects including increased muscle strength and power, improved balance, improved blood circula-tion, improved bone mineral density, improved health-related quality of life, and hormonal fluctuations (e.g. growth hormone, IGF-1, cortisol, and testosterone) resul-ting from WBV exposure (Gómez-Cabello et al., 2012; Prisby et al., 2008; Bruyere et al., 2005; Jordan et al., 2005; Cardinale and Wakeling, 2005; Cardinale and Bosco, 2003).
Cardinale and Bosco (2003) report that vibration was first utilized as an exercise intervention by Russian scientists in the mid 1980’s. More recently, whole body vibration training (WBVT) has been utilized both scien-tifically and recreationally using commercially available platforms designed to produce sinusoidal vibrations of adjustable frequency and amplitude. While there appears to be mixed evidence regarding the ability of WBVT to stimulate a significant cardiovascular response (Jordan et al., 2005), some have concluded that WBVT can elicit cardiovascular and metabolic responses in some people similar to other forms of mild exercise (Cardinale and Wakeling, 2005). Because of its wide range of potential physiological benefits, and because it can be applied in a relatively low-effort, low-impact manner with no complica-ted technique to learn, some have suggested that WBVT may be of particular benefit to the elderly and special populations characterized by impaired mobility (e.g. patients with stroke, Parkinson’s disease, osteoporosis, or arthritis) (Prisby et al., 2008; Cardinale and Wakeling, 2005; Cardinale and Bosco, 2003; Arias et al., 2009; Pinto et al., 2010).
In vitro studies have been conducted that suggest that vibration may have a beneficial effect on cartilage synthe-sis (Liu et al., 2001; Takeuchi et al., 2006). Mechanical loading, such as vibration, may regulate chondrocyte function through some yet to be determined pathway, and suggested the possible involvement of chondrocyte cell surface receptors for certain cartilaginous extracellular matrix (ECM) molecules (Liu et al., 2001). Takeuchi et al. (2006) found that, in cultured chondrocytes, vibration significantly increased the synthesis of chondroitin sulfate, an ECM component, and that the effect was even greater in the presence of hyaluronic acid (HA). They also reported increased expression of proteins involved in the intracellular signal transduction system in groups of chondrocytes treated with vibration. An additional proposed benefit from this study is improved nutrient delivery and waste removal among chondrocytes as a result of a more even distribution of HA and movement of the ECM, caused by vibration.
Despite these interesting and promising findings, it must be noted that in terms of frequency, amplitude, and duration, the vibration parameters applied in these set-tings were quite different than what is typically applied in human populations. Furthermore, no evidence of similar beneficial effects exists in vivo, and the long-term effect of WBV on articular cartilage is still unknown (Prisby et al., 2008). Nevertheless, the existence of a safe and efficient stimulus to combat the effects of aging on chondrocytes would be groundbreaking in the treatment of OA.
AIM OF THE STUDY
In this study, the terms arthritis, arthrosis, osteoarthrosis and osteoarthritis will be used to characterize disorders associated with the AC. As no previous systematic reviews of the effects of WBV exercise on people with OA have been published, the purpose of this study was to review published research concerning the use of WBV in people with OA using PubMed and Scopus databases.
METHODOLOGY
Databases used in this study
PubMed and SciVerse Scopus online databases were searched on the 13th of June 2014. PubMed comprises more than 23 million citations for biomedical literature from MEDLINE, life science journals, and online books (http://www.ncbi.nlm.nih.gov/pubmed).
SciVerse Scopus is the world’s largest abstract and citation database of peer-reviewed literature and quality web sources. It contains 53 million records, 70% with abstracts, nearly 21,915 titles from 5,000 publishers worldwide (http://www.info.sciverse.com/scopus/about).
Search strategy used to find the publications involving WBV and clinical articular diseases
Searches were performed using the keywords: (i) arthrosis, (ii) arthrosis and “whole body vibration”, (iii) osteoarthrosis, (iv) osteoarthrosis and “whole body vibration”, (v) arthritis, (vi) arthritis and “whole body vibration”, (v) osteoarthritis, (vi) osteoarthritis and “whole body vibration”, (vii)
arthrosis and “vibratory platform”, (viii) arthritis and “vibratory platform”, (ix) osteoarthrosis and “vibratory platform”, (x) osteoarthritis and “vibratory platform”, and (xi) arthrosis and “oscillating platform”, (xii) arthritis and “oscillating platform”, (xiii) osteoarthrosis and “oscillating platform”, (xiv) osteoarthritis and “oscillating platform”.
Inclusion and exclusion criteria to select the publications
Papers were included for review if they met the search criteria and described a study using whole body vibration generated by an oscillating platform used to treat people with clinical articular diseases and the paper was available only in English. Review articles, case reports and investigations only with healthy subjects were excluded. Papers about the effect of the occupational use of the vibration in workers and involving studies with animals were also deleted. Investigations performed involving whole body vibration and other therapeutic procedures were not considered to be analysed.
Data were independently abstracted by the authors and disagreements were resolved by consensus of, at least, three co-authors.
RESULTS
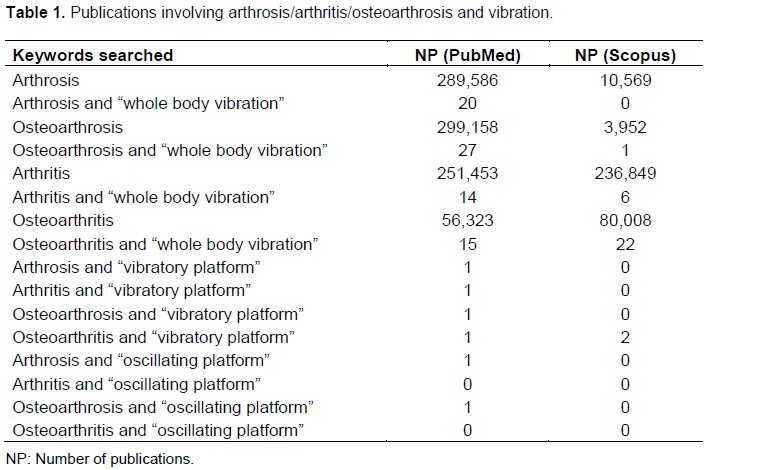
Table 1 shows the number the publications (NP) found with the keywords when they were searched in PubMed and Scopus databases. In PubMed, NP using the key-words arthrosis, osteoarthrosis and arthritis was almost the same. Considering the Scopus database, intriguingly, NP was extremely lower to arthrosis and osteoarthrosis; however, NP with the keyword arthritis is closed to PubMed. The search using the keywords involving articular disorders (osteoarthrosis or osteoarthritis or arthrosis or arthritis) and source of vibration (“whole body vibration”, “oscillating platform”, “vibratory platform”) yielded 82 publications in PubMed and 31 publications in Scopus.
The four selected English language publications found with keywords "whole body vibration" and some terms related to articular disorders that reached all the inclusion criteria were analyzed. Descriptions of the type of platform, the subjects (number, sex and age), the frequency and the amplitude used in the platforms used in these 4 studies are as shown in Table 2.
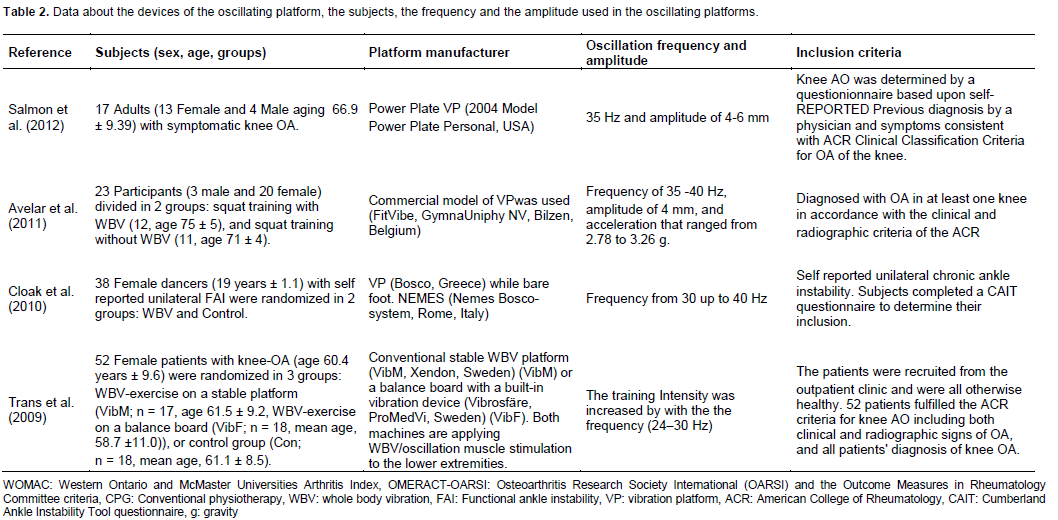
Putting together the information found in the analyzed four papers, the number of subjects ranged from 15 to 52. Moreover, the frequencies used in the studies ranged from 24 to 40 Hz. The self-report of the status of disease (WOMAC) was used in 2 papers (Trans et al., 2009; Avelar et al., 2011) while pain levels were evaluated by the visual analog scale (VAS) in 2 papers (Cloak et al., 2010; Salmon et al., 2012). Different tests were used in these studies, as (i) TUG, (ii) step test, (iii) 20 m walk test (Salmon et al., 2012), (iv) timed get up and go test (TGUG), (v) chair stand test (CST), (vi) 6-minute walk test (6MWT), (Avelar et al., 2010), (vii) knee muscle strength (extension/flexion) and (viii) proprioception (threshold for detection of passive movement (TDPM) to evaluate the effects promoted by the exercises due to the WBV (Trans et al., 2009).
DISCUSSION
Osteoarthritis, arthritis, arthrosis and osteoarthrosis are terms that have been used in studies related to the clinical disorders associated with the articular cartilages (Lievense et al., 2002). However, when these terms are used as keywords in searches in different databases, we found an intriguing result. Using the keyword arthrosis, only 10,569 references were found in the Scopus database, while 289,586 were found in the PubMed. A similar finding was observed when the keyword osteoarthrosis was used. When these keywords arthritis and osteoarthritis were used in the searches, the number of publications in both databases was similar. As Scopus and Pubmed are important databases, these findings can be relevant to aid in a discussion about the keywords that must be used to try to find references about arthropathy.
Searches using the different words related with arhrosis and WBV revealed a reduced number of publications, although WBV is widely available to exercisers and patients, as well as the fact that it is used to treat various musculoskeletal and neurological disorders (Schuhfried et al., 2005; Wunderer et al., 2010). Rittweger (2010) reported that it appears as if this modality is still unknown to the scientific community and our findings seem to confirm this belief. The number of publications about the effects and applications of the WBV has increased strongly in the last three years, as it is possible to see in the databases used in this study.
Review articles, case reports, investigations only with healthy subjects, papers about the effect of the occupational use of the vibration in workers and involving studies with animals, investigations performed involving whole body vibration and other therapeutic procedure were not considered to be discussed (Osugi et al., 2014; Park et al., 2013; Gómez-Cabello et al., 2012; Melnyk ett al., 2009; Melnyk et al., 2008).
Following the exclusion criteria, only four papers could be selected for discussion in the current work (Trans et al., 2009; Avelar et al., 2011; Cloak et al., 2010; Salmon et al., 2012). Concerning to the use of WBV in patients with osteoarthrosis, the number of publications found in the databanks varied (17 to 52 subjects). As it would be expected, due to the prevalence of this disease (Lawrence et al., 2008), the number of females in the investigations is greater than the number of males. All the authors have reported positive effects of the WBV (Trans et al., 2009; Avelar et al., 2011; Cloak et al., 2010; Salmon et al., 2012) with improvements of some clinical function in patients with osteoarthitis. An important feeling in this revision is that although the number of the studies is small, they may constitute first hints for the efficacy of WBV in the treatment of the osteoarthrosis.
In addition, in general, exercise therapy has been con-sidered to be an important and supportive treatment for people with musculoskeletal disorders (French et al., 2013). WBV exercises are performed in oscillating plat-forms, and Madou and Croni (2008) have reviewed the effects of WBV on physical and physiological capability in special populations and they concluded that WBV provides alternative and/or additional therapeutic interventions to improve physical and functional performance. The specific loading parameters and the value of WBV as compared with conventional interventions need to be the source of future research.
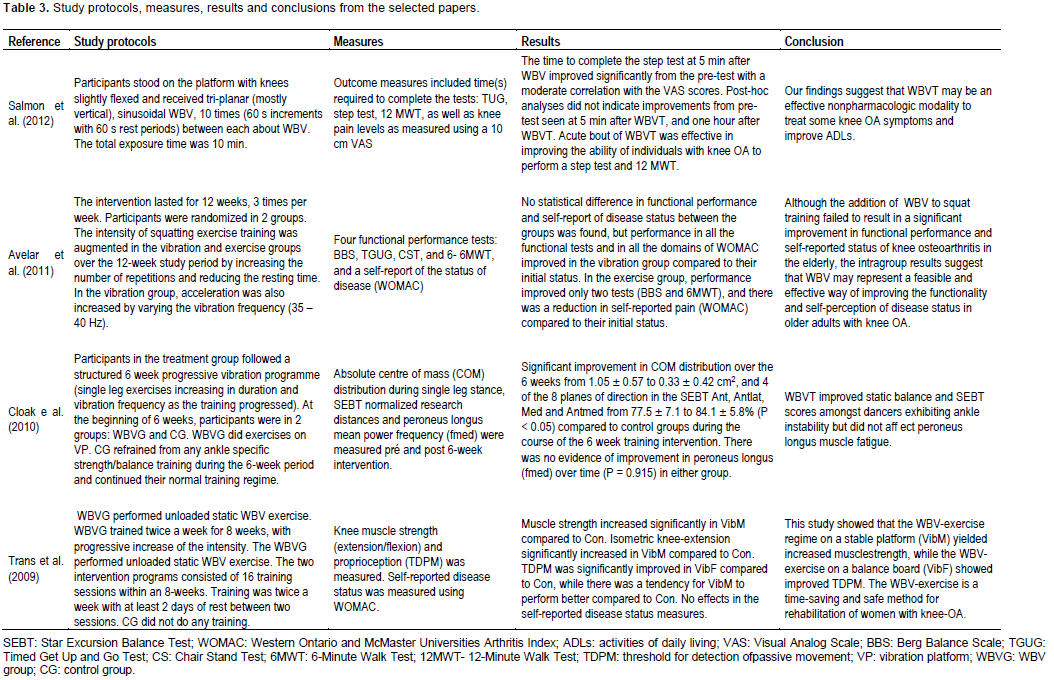
OA is associated with multiple impairments of muscle and articular functions, balance and pain that cause a de-crease of the quality of life of the subject (van den Berg, 2010; ACR, 2013; ORSI, 2013). In addition, there is no cure to this disease and, concerning to non-pharmacologic and non-invasive therapy, the aim of the treatment is to optimize and to improve the neuro-muscular and articular functions, as well as to increase the muscular strength. With these purposes, the vibrations generated in the oscillating/vibratory platforms would expected that WBV exercises would seem an important alternative to the management of patients with osteoarthrosis due to some benefits related to the action in the muscle performance reported in the papers presented as shown in Table 3. Salmon et al. (2012) have reported that the time to complete the step test at 5 min after the WBV improved significantly from the pretest with a moderate correlation with the VAS scores. Avelar et al. (2011) found that the performance of patients in all the functional tests (BBS, TGUT, CST and 6MWT) and in all domains of the WOMAC have improved in the group submitted to the WBV. Cloak et al. (2009) demonstrated that the absolute centre of mass distribution has improved over 6 weeks due to the WBV. Trans et al. (2009) reported that in the patients with osteoarthrosis, the muscle strength and knee-extension significantly increased due to the WBV.
The potential mechanisms by which WBV improves neuromuscular performance and pain are not well understood, although a few theories on how WBV can stimulate the neuromuscular system have emerged. It is extensively theorized that the WBV stimulus causes short and rapid changes in muscle fiber length which result in skeletal muscle reflex contractions (Ritzmann et al., 2010). These reflexive contractions result in an increased neuromuscular load placed on the muscle (Roelants et al., 2006). On the other hand, another mechanism could be the proprioceptive feedback potentiation of inhibition of pain by vibration receptors in the skin stimulate inhibitory interneurons in the spinal cord, which in turn act to reduce the amount of pain signal transmitted from A-δ and C fibers across the midline of the spinal cord and from there to the brain (Melzack and Wall, 1965). This mechanism increases pain threshold (Lunoeberg et al., 1987). This could explain how WBV applied to the lower limbs could improve VAS scores.
In conclusion, the number of publications found in the databases searched involving WBV and osteoarthrisis is small, and, in general, the protocols are different. In addition, the number of publications about the effects and applications of the WBV has increased strongly in the last the last three years. The analysis of the findings of these studies indicates that the WBV could bring some benefits to patients with OA. In addition, we suggest further larger scale investigations with controlled parameters and well designed protocols into the effects of WBV exercises in people with osteoarthrois. This would be highly desired to improve the quality of life of the patients with this disease, decreasing pain and the medications, as well as to avoid surgery.
ABBREVIATIONS
OA, Osteoarthritis; ECM, cartilaginous extracellular matrix; NP, number of publications; NSAIDs, nonsteroidal antiinflammatory drugs; ROM, range of motion; WBV, whole body vibration; WBVT, whole body vibration training.
REFERENCES
| Abercromby AF, Amonette WE, Layne CS, McFarlin BK, Hinman MR, Paloski WH (2007). Vibration exposure and biodynamic responses during whole-body vibration training. Med. Sci. Sports Exerc. 39:794-800. crossref | ||||
| American College of Rheumatology (2013). http://www.rheumatology.org Acessed June 24, 2013. | ||||
| Arias P, Chouza M, Vivas J, Cudeiro J (2009). Effect of whole body vibration in Parkinson's disease: a controlled study. Mov. Disord. 24:891-898. crossref | ||||
| Arokoski JP, Jurvelin JS, Väätäinen U, Helminen HJ (2000). Normal and pathological adaptations of articular cartilage to joint loading. Scand. J. Med. Sci. Sports 10:186-198. crossref | ||||
| Avelar NCB, Prado Simão AP, Tossige-Gomes R, Neves CDC, Rocha-Vieira E, Coimbra CC, Lacerda ACR (2011). The Effect of Adding Whole-Body Vibration to Squat Training on the Functional Performance and Self-Report of Disease Status in Elderly Patients with Knee Osteoarthritis: A Randomized, Controlled Clinical Study. J. Altern. Complement. Med. 17:1149-1155. crossref | ||||
| Bijlsma JW, Berenbaum F, Lafeber FP (2010). Osteoarthritis: an update with relevance for clinical practice. Lancet 377:2115-2126. crossref | ||||
| Bruyere O, Wuidart MA, Di Palma E, Gourlay M, Ethgen O, Richy F, Reginster JY (2005). Controlled whole body vibration to decrease fall risk and improve health-related quality of life of nursing home residents. Arch. Phys. Med. Rehabil. 86:303-307. crossref | ||||
| Cardinale M, Bosco C (2003). The use of vibration as an exercise intervention. Exerc. Sport. Sci. Rev. 31:3-7. crossref | ||||
| Cardinale M, Wakeling J (2005). Whole body vibration exercise: are vibrations good for you? Br. J. Sports Med. 39:585-589. crossref | ||||
| Charlton DC, Peterson MGE, Spiller K, Lowman A, Torzilli PA, Maher SA (2008). Semi-Degradable Scaffold for Articular Cartilage Replacement. Tissue Eng. Part. A. 14:207-213. crossref | ||||
| Cloak R, Nevill AM, Clarke F, Day S, Wyon MA (2010). Vibration training improves balance in unstable ankles. Int. J. Sports Med. 31:894-900. crossref | ||||
| Eyre DR, Weis MA, Wu JJ (2006). Articular cartilage collagen: an irreplaceable framework? Eur. Cell. Mater. 12:57-63. pubmed | ||||
| French HP, Cusack T, Brennan A, Caffrey A, Conroy R, Cuddy V, FitzGerald OM, Gilsenan C, Kane D, O'Connell PG, White B, McCarthy GM (2013). Exercise and manual physiotherapy arthritis research trial (EMPART) for osteoarthritis of the hip: a multicenter randomized controlled trial. Arch. Phys. Med. Rehabil. 94:302-314. crossref | ||||
| Gillogly SD, Voight M, Blackburn T (1998). Treatment of articular cartilage defects of the knee with autologous chondrocyte implantation. J. Orthop. Sports Phys. Therapy 28:241-251. crossref | ||||
| Goldring MB, Goldring SR (2007). Osteoarthritis. J. Cell. Physiol. 213:626-634. crossref | ||||
| Gómez-Cabello A, Ara I, González-Agüero A, Casajús JA, Vicente-Rodríguez G (2012). Effects of training on bone mass in older adults: a systematic review. Sports Med. 42:301-325. crossref | ||||
| Goodwin JL, Kraemer JJ, Bajwa ZH (2005). The use of opioids in the treatment of osteoarthritis: when, why, and how? Curr. Pain Headache Rep. 9:390-398. crossref | ||||
| Haas SB, Barrack RL, Westrich G, Lachiewicz PF (2008). Venous thromboembolic disease after total hip and knee arthroplasty. J. Bone Joint Surg. Am. 90:2764-2780. Pubmed | ||||
| Jordan MJ, Norris SR, Smith DJ, Herzog W (2005). Vibration training: an overview of the area, training consequences, and future considerations. J. Strength Cond. Res. 19:459-466. crossref | ||||
| Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, Gabriel S, Hirsch R, Hochberg MC, Hunder GG, Jordan JM, Katz, JN, Kremers HM, Wolfe F (2008). Estimates of the Prevalence of Arthritis and Other Rheumatic Conditions in the United States. Part II. Arthritis Rheum. 58:26-35. crossref | ||||
| Lingard EA, Riddle DL (2007). Impact of psychological distress on pain and function following knee arthroplasty. J. Bone Joint Surg. Am. 89:1161-1169. crossref | ||||
| Lievense AM, Bierma-Zeinstra SMA, Verhagen AP, van Baar ME, Verhaar JAN, Koes BW (2002). Influence of obesity on the development of osteoarthritis of the hip: a systematic review. Rheum. 41:1155-1160. crossref | ||||
| Lings S, Leboeuf-Yde C (2000). Whole-body vibration and low back pain: a systematic, critical review of the epidemiological literature 1992-1999. Int. Arch. Occup. Environ. Health 73:290-297. crossref | ||||
| Liu J, Sekiya I, Asai K, Tada T, Kato T, Matsui N (2001). Biosynthetic response of cultured articular chondrocytes to mechanical vibration. Res. Exp. Med. 200:183-193. | ||||
| Loeser RF (2006). Molecular mechanisms of cartilage destruction: Mechanics, inflammatory mediators, and aging collide. Arthritis Rheum. 54:1357-1360. crossref | ||||
| Lunoeberg TP, Abrahamsson L, Bondesson L, Hak-Kr E (1987). Vibratory stimulation compared to placebo in alleviation of pain. Scand. J. Rehabil. Med. 19:153-158. | ||||
| Madou KH, Cronin JB (2008). The effects of whole body vibration on physical and physiological capability in special populations. Hong Kong Physiother. J. 26:24-38. crossref | ||||
| Melnyk M, Kofler B, Faist M, Hodapp M, Gollhofer A (2008). Effect of a whole-body vibration session on knee stability. Int. J. Sports Med. 29:839-844. crossref | ||||
| Melnyk M, Schloz C, Schmitt S, Gollhofer A (2009). Neuromuscular ankle joint stabilisation after 4-weeks WBV training. Int. J. Sports Med. 30:461-466. crossref | ||||
| Melzack R, Wall PD (1965). Pain mechanisms: a new theory. Science 150:971-979. crossref | ||||
| Meulenbelt I, Kloppenburg M, Kroon HM, Houwing-Duistermaat JJ, Garnero P, Hellio-Le Graverand MP, DeGroot J, Slagboom PE (2007). Clusters of biochemical markers are associated with radiographic subtypes of osteoarthritis (OA) in subject with familial OA at multiple sites. The GARP study. Osteoarthr. Cartil. 15:379-385. crossref | ||||
| Miehle W (1987). Arthrosis or osteoarthritis: do these terms imply therapy with pure analgesics or non-steroidal antirheumatic agents? Scand. J. Rheumatol. Suppl. 65:123-130. crossref | ||||
| National Institute of Arthritis and Musculoskeletal and Skin Diseases (2013). Osteoarthritis http://www.niams.nih.gov/Health_Info/Osteoarthritis/default.asp Accessed June 23, 2013. | ||||
| Osteoarthritis Research Society International (2013). http://www.oarsi.org/, acessed in June 24, 2013 | ||||
| Osugi T, Iwamoto J, Yamazaki M, Takakuwa M (2014). Effect of a combination of wholebody vibration exercise and squat training on body balance, muscle power, and walking ability in the elderly. Ther Clin Risk Manag. 10:131-138. | ||||
| Park YG, Kwon BS, Park JW, Cha DY, Nam KY, Sim KB, Chang J, Lee HJ (2013). Therapeutic effect of whole body vibration on chronic knee osteoarthritis. Ann. Rehabil. Med. 37:505-515. crossref | ||||
| Patella V, Speciale D, Patella S, Moretti B, Pesce V, Spinarelli A (2008). Wound necrosis after total knee arthroplasty. Orthopedics 31:807-808. crossref | ||||
| Peat G, McCarney R, Croft P (2001). Knee pain and osteoarthritis in older adults: a review of community burden and current use of primary health care. Ann. Rheum. Dis. 60:91-97. crossref | ||||
| Pinto NS, Monteiro MB, Meyer PF, Santos-Filho SD, Azevedo-Santos F, Bernardo RM, Paiva D, Thompson D, Missailidis S, Marín PJ, Haas CT, Bernardo-Filho M (2010). The effects of whole-body-vibration exercises in Parkinson’s disease: a short review. J. Med. Med. Sci. 2:594-600. | ||||
| Prisby RD, Lafage-Proust M, Malaval L, Belli A, Vico L (2008). Effects of whole body vibration on the skeleton and other organ systems in man and animal models: what we know and what we need to know. Ageing Res. Rev. 7:319-329. crossref | ||||
| Reginster JY (2002). The prevalence and burden of arthritis. Rheumatology 41:3-6. crossref | ||||
| Rittweger J (2010). Vibration as an exercise modality: how it may work, and what its potential migth be. Eur. J. Appl. Physiol. 108:877-904. crossref | ||||
| Ritzmann R, Kramer A, Gruber M, Gollhofer A, Taube W (2010). EMG activity during whole body vibration: motion artifacts or stretch reflexes? Eur. J. Appl. Physiol. 110:143-151. crossref | ||||
| Roelants M, Verschueren SM, Delecluse C, Levin O, Stijnen V (2006). Whole-body-vibration-induced increase in leg muscle activity during different squat exercises. J. Strength Cond. Res. 20:124-129. crossref | ||||
| Salmon JR, Roper JA, Tillman MD (2012). Does Acute Whole Body Vibration Training Improve the Physical Performance of People With Knee Osteoarthritis? J. Strength Cond. Res. 26:2983-2989. crossref | ||||
| Schroeppel JP, Crist JD, Anderson HC, Wang J (2011). Molecular regulation of articular chondrocyte function and its significance in osteoarthritis. Histol. Histopathol. 26:377-394. pubmed | ||||
| Schuhfried O, Mittermaier C, Jovanovic T, Pieber K, Paternostro-Sluga T (2005). Effects of whole-body vibration in patients with multiple sclerosis: a pilot study. Clin. Rehabil. 19:834-842. crossref | ||||
| Seidel H (1993). Selected health risks caused by long term whole body vibration. American J. Ind. Med. 23:589-604. crossref | ||||
| Stein G, Knoell P, Faymonville C, Kaulhausen T, Siewe J, Otto C, Eysel P, Zarghooni K (2010). Whole body vibration compared to conventional physiotherapy in patients with gonarthrosis: a protocol for a randomized, controlled study. BMC Musculoskelet. Disord. 11:128-129. crossref | ||||
| Takeuchi R, Saito T, Ishikawa H, Takigami H, Dezawa M, Ide C, Itokazu Y, Ikeda M, Shiraishi T, Morishita S (2006). Effects of vibration and hyaluronic acid on activation of three-dimensional cultured chondrocytes. J. Arthritis Rheum. 54:1897-1905. crossref | ||||
| Trans T, Aaboe J, Henriksen M, Christensen R, Bliddal H, Lund H (2009). Effect of whole body vibration exercise on muscle strength and proprioception in females with knee osteoarthritis. Knee 16:256-261. crossref | ||||
| van den Berg WB (2010). Osteoarthritis year 2010 in review: pathomechanisms. Osteoarthr. Cartil. 19:338-341. crossref | ||||
| Wang M, Shen J, Jin H, Im H, Sandy J, Chen D (2011). Recent progress in understanding molecular mechanisms of cartilage degeneration during osteoarthritis. Ann. N.Y. Acad. Sci. 1240:61-69. crossref | ||||
| Webb BG, Lichtman DM, Wagner RA (2008). Risk factors in total joint arthroplasty: comparison of infection rates in patients with different socioeconomic backgrounds. Orthopedics 31:445-446. PMid:19292321 | ||||
| Wu JJ, Weis MA, Kim LS, Eyre DR (2011). Type III collagen, a fibril network modifier in articular cartilage. J. Biol. Chem. 285:18537-18544. crossref | ||||
| Wunderer K, Schabrun SM, Chipchase L (2010). Effects of whole body vibration on strength and functional mobility in multiple sclerosis. Physiother. Theory Pract. 26:374-384. crossref | ||||
| Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M, Dougados M, Hochberg M, Hunter DJ, Kwoh K,Lohmander LS, Tugwell P (2008). OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr. Cartil. 16:137-162. crossref | ||||
Похожие статьи
Цаликова Ида Константиновна
Пахотина Светлана Владимировна