This article is published under a Creative Commons license and not by the author of the article. So if you find any inaccuracies, you can correct them by updating the article.

Applying Automated Working Memory Assessment and Working Memory Rating Scale in Russian Population



Kseniya Absatova
Published: April 1, 2016
Latest article update: Sept. 16, 2022
This article is published under the license




Abstract
In the current study, two standardized English-language assessments, the AWMA by T.P. Alloway (2007) and the WMRS (Alloway, Gathercole, & Kirkwood, 2008), were translated into Russian. The translated version of the AWMA was undertaken by 51 adults and 73 primary school children, and the translated version of the WMRS was completed by the teachers who worked with those children. The WMRS is a questionnaire list for teachers with 20 items which describe possible behavior manifestations of poor working memory in the classroom. The AWMA is a computer test battery with 12 subtests which aim to assess verbal short-term memory, verbal working memory, visuospatial short-term memory and visuospatial working memory. The performance of participants in the Russian sample was compared with the normative sample and an almost identical pattern of results was observed. This study is the first trial of the AWMA and the WMRS application in a Russian-speaking population.
Keywords
Working memory, Automated Working Memory Assessment (AWMA), assessment, adults, Working Memory Rating Scale (WMRS), primary school children
Introduction
Working memory (WM) refers to the ability to retain relevant information while completing a cognitive task. Within the framework of the most widely accepted WM model proposed by Baddeley and Hitch (1974), this ability relies upon a multicomponent system responsible for the maintenance and simultaneous processing of necessary information during short periods of time (Baddeley & Hitch, 1974; Baddeley, 1992; 2010). WM is involved in almost every kind of routine activity and experiences progressive changes during development, especially between the period of 5 to 19 years of age (Alloway & Alloway, 2013). It is independent of socioeconomic background, including the mother’s educational level, number of years in preschool, etc. (Engel de Abreu, Santos, & Gathercole, 2008; Alloway, Alloway, & Wootan, 2014) and has been linked to a number of cognitive skills important for successful learning (Bayliss, Jarrold, Gunn, & Baddeley, 2003; Gathercole, Alloway, Willis, & Adams, 2006; Alloway & Copello, 2013; Chryso- choou, Masoura, & Alloway, 2013). Some studies showed its impact and predictive potential for learning outcomes (Gathercole, Lamont, & Alloway, 2006; Alloway, 2009; Alloway & Alloway, 2010).
Among the existing methods of WM assessment, there are two widely applied standardized tools developed on the basis of Baddeley’s working memory model. The first is the Working Memory Rating Scale (WMRS), a behavioral rating scale for teachers developed in order to easily identify children aged 5-11 with poor working memory (Alloway, Gathercole, & Kirkwood, 2008). It was developed using interviews with teachers who were observing children with both low and average WM skills. These observations were reviewed, and after selecting those most sensitive to WM deficits, were rated for behavior typicality in four gradations ranging from “not typical at all” to “very typical”. It takes approximately five minutes to complete the questionnaire; results are easily interpreted and may include a recommendation to administer a detailed working memory assessment if a child is at risk of poor educational progress. The WMRS is considered to be a reliable screening tool (Alloway, Gathercole, Kirkwood, & Elliott, 2009; Normand & Tannock, 2014) and has been translated and adapted in several countries (Alloway, Gathercole, & Kirkwood, 2008; Engel de Abreu, et al., 2014; Politimou, Masoura, & Kiosseoglou, 2015).
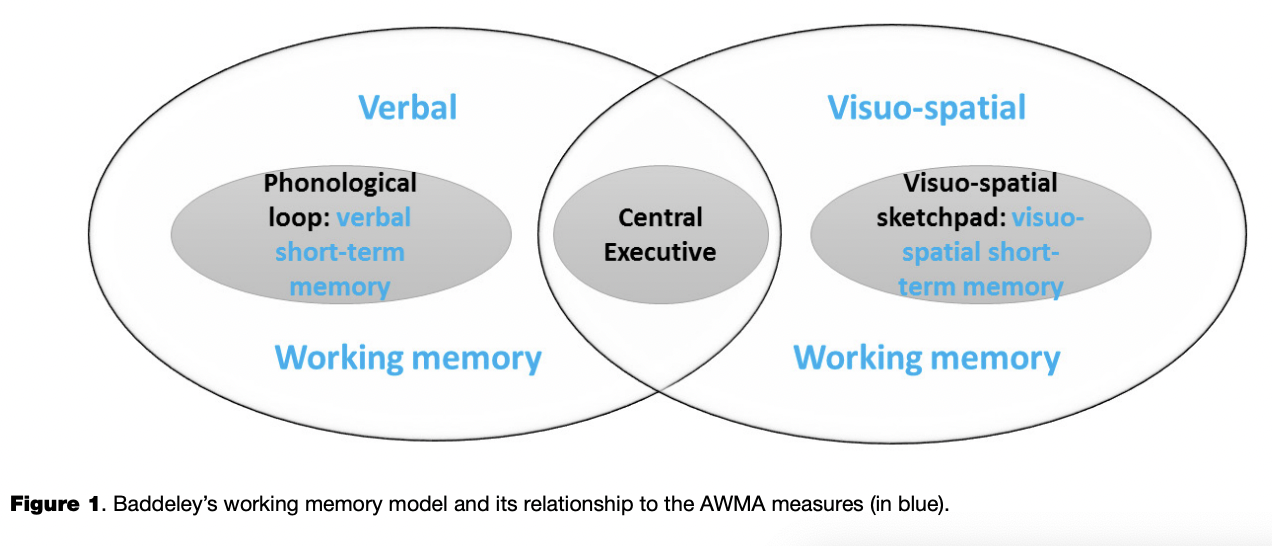
The other standardized and validated method is the Automated Working Memory Assessment (AWMA), a computer test battery of WM skills assessment for individuals from 4 to 22 years of age (Alloway, 2007; Alloway, Gathercole, Kirkwood, & Elliott, 2008). The AWMA includes four measures of active and passive WM storage, each of which can be assessed by three corresponding subtests: verbal short-term memory (the Digit Recall subtest, the Word Recall subtest, the Nonword Recall subtest), verbal working memory (the Listening Recall subtest, the Backward Digit Recall subtest, the Counting Recall subtest), visuospatial short-term memory (the Mazes Memory subtest, the Block Recall subtest, the Dot Matrix subtest) and visuospatial working memory (the Odd One Out subtest, the Mr. X subtest, the Spatial Recall subtest).
As illustrated by Figure 1, the WM model developed by Baddeley and Hitch (Baddeley & Hitch, 1974) includes three main components: the phonological loop, the visuospatial sketchpad and the central executive. While the visuospatial sketchpad and the phonological loop can be considered as passive or short-term memory storages for visuospatial and verbal information respectively, the central executive is involved in active or working memory storage, which requires not only the ability to retain information held in passive storages but also to manipulate it.
There are three versions of AWMA administration: the AWMA Screener, consisting of two tests and suitable for screening when working memory deficits are suspected; the AWMA Short Form, consisting of four tests and recommended when WM difficulties are suspected but their specificity is unknown; and the AWMA Long Form, consisting of all 12 tests for a detailed assessment. The AWMA has been translated into more than ten languages (e.g., Injoque-Ricle, Calero, Alloway, & Burin, 2011) and applied in groups of individuals with atypical development, such as dyslexia (Alloway, Wootan, & Deane, 2014), specific language impairment (Alloway, Rajendran, & Archibald, 2009; Alloway & Stein, 2014), developmental coordination disorder (Alloway & Temple, 2007; Alloway, Rajendran, & Archibald, 2009; Alloway, 2011; 2012), attention deficit hyperactivity disorder (Alloway, Rajendran, & Archibald, 2009; Alloway, 2011; Alloway & Stein, 2014; Holmes, et al., 2014) and autistic spectrum disorders (Alloway, Rajendran, & Archibald, 2009).
Unfortunately, there are no standardized methods of working memory assessment for Russian speakers. Even the Wechsler Intelligence Scale for Children Fourth Edition (WISC-VI), which had included a separate working memory measure (Working Memory Index) since 2003 (Wechsler, 2003), has not been adapted in Russian yet, while the previous versions of the WISC are widely applied in Russia. Motivated by this fact, the current study aimed at drawing the attention of specialists to the possibility of applying the two standardized methods in the Russian population.
Method
Participants
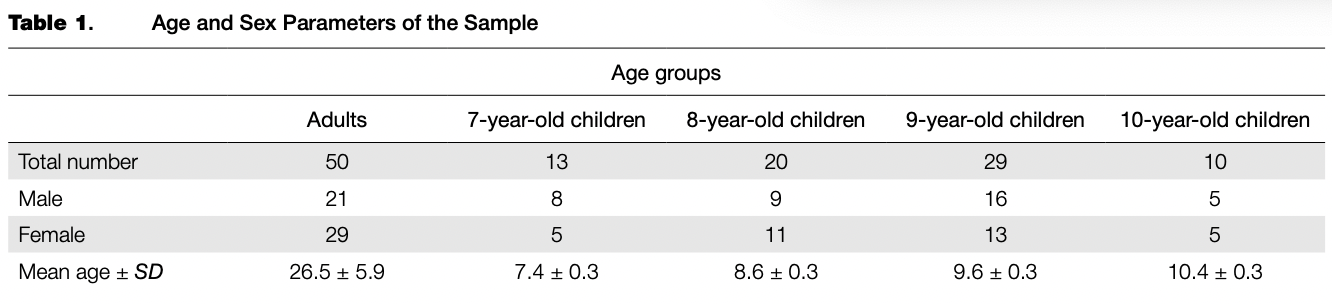
Fifty adults and seventy-two primary school children participated in the adaptation. Informed consent was obtained from the adult participants and the parents of the underage children. Adults were between the ages of 18 and 48 years; children belonged to four age groups, as shown in Table 1. Children who participated in the study attended a public Moscow school (the 1st, the 2nd or the 3rd year). None of the participants had any history of psychiatric or neurological impairments nor had any repeated any courses. Six teachers who had been working with the children filled in WMRS questionnaire forms. Along with the above normative sample, the following two cases were studied: a child with pronounced learning difficulties and an adult with memory impairments volunteered to participate in the experiment. Their data were separately analyzed and are described in the Results section.
Procedure
Adult participants completed all 12 subtests in the same order pre-arranged by the AWMA computer program. Children completed 8 tests in the following order: the Digit Recall subtest, the Listening Recall subtest, the Odd One Out subtest, the Word Recall subtest, the Mazes Memory subtest, the Mr. X subtest, the Block Recall subtest and the Backward Digit Recall subtest. It took approximately 90 minutes to complete the battery for adults and about 35-45 minutes for children. The subtests always started with their first trials and were preceded by practice trials.
During the administration of the AWMA subtests, each participant’s response was compared with the correct one provided in the AWMA Scorebook (Alloway, 2007) and entered with a keyboard using a simple yes/no schema. Next, the raw scores of the subtests were processed by the program and exported into individual reports. Besides a separate file with individual raw scores, a report generated by the AWMA program contained personal information (including age at testing), scores standardized to a mean of 100 and a standard deviation of 15 points for each age band (standard scores), percentiles, and a graph with composite scores for each AWMA measure (for an example, see Case Study 1, Case Study 2 or visit http://www.pearsonclinical.co.uk/). The report provided a learning profile with brief information about each memory component, individual performance in this area and learning difficulties if any.
Measures
Automated working memory assessment. Verbal short term memory subtests. The Digit Recall subtest, the Word Recall subtest and the Nonword Recall subtest consisted of orally presented sequences of digits, words and nonwords respectively. The Digit Recall started with a block of 1 digit and increased to a block of 9 digits. The Word Recall started with a block of 1 word and increased to a block of 7 words. The Nonword Recall started with a block of 1 nonword and increased to a block of 6 nonwords. Each block included six trials (this was true for all subtests in the battery). A participant should immediately recall each of the presented sequences in the correct order.
Verbal working memory subtests. In the Listening Recall subtest, a participant heard a sequence of sentences (e.g., “Dogs have four legs”) and at the end of each sentence judged if it was true or false. Then, at the end of each trial, after the judgement of all sentences in a sequence, she/ he should recall the final words of each sentence exactly in the same order as they had been presented (e.g., “legs”). The subtest began with a block of 1 sentence and increased to a block of 6 sentences. In the Counting Recall subtest, a participant counted aloud a number of red circles in a sequentially presented visual arrays of circles and triangles (e.g., the first array counts: “1,2,3,4”; the second array counts: “ 1,2,3,4,5,6,7”) and at the end of each block he or she should immediately recall the total number of red circles calculated in each array exactly in the same order as they had been presented (e.g., “4 and 7”). The subtest began with a block of 1 array and increased to a block of 7 arrays of circles and triangles. In the Backward Digit Recall, a participant heard a sequence of digits and then immediately recalled each sequence in backwards order. The subtest started with a block of 2 digits and increased to a block of 7 digits.
Visuospatial short term memory subtests. In the Dot Matrix subtest, a participant was shown the sequential positions of a red dot in a four-by-four squared matrix (the red dot sequentially appeared in different locations of a blank squared matrix), and at the end of the block he or she should tap all those squares (locations) on the blank matrix exactly in the same order as the red dot was presented. The subtest began with a block of 1 dot and increased to a block of 9 dots. The Mazes Memory subtest is a presentation of a way out of a maze (a red line path). A participant should remember this path and trace it with her/his finger on the same (but blank) maze presented three seconds later on the computer screen. The subtest began with small simple mazes and increased to large complex mazes. In the Block Recall subtest, a participant viewed a 3D board with randomly arranged blocks. A finger sequentially taps different blocks and then a participant should point at the same blocks in the same order as they were tapped during the presentation. The subtest began with a block of 1 block and increased to a block of 9 blocks.
Visuospatial working memory subtests. In the Odd One Out subtest, participants were sequentially presented with sets of three geometrical shapes arranged one by one in three squared frames. Two of these three shapes are absolutely identical and the third is different. During the presentation of each set of shapes, a participant should identify and point at an odd-one-out shape and remember its location (the left, the middle, or the right frame). After the presentation of all sets in the block, all the locations of each odd-one-out shape should be recalled exactly in the same order as the sets were presented. The subtest began with a block of 1 set of shapes and increased to a block of 7 sets of shapes. The Mr. X subtest involves a simultaneous presentation of two Mr. X figures. The left Mr. X is always in a yellow hat, standing on his legs and holding a ball in his right or left hand. The right Mr. X is always in a blue hat, holding a ball in his right or left hand, and his body may be rotated clockwise or counterclockwise taking six different orientations; thus, the ball he holds can be found in six different locations. During each presentation of the two Mr. X figures, a participant should identify if Mr. X in the blue hat is holding his ball in the same hand as Mr. X in the yellow hat and remember the location of the ball which Mr. X in the blue hat holds. A block of trials starts with a presentation of 1 pair of Mr. X figures and increases to the sequential presentation of 7 pairs of Mr. X figures. After a block of trials, participants should recall each location of the balls which Mr. X in the blue hat held by pointing at the picture with six possible locations marked. In the Spatial Recall subtest, a participant is presented with a pair of identical shapes, in which a right shape has a red dot above it and is rotated clockwise or counterclockwise. During the presentation, they should identify weather the shape with the red dot is the same or the opposite of the other shape. The shape with the red dot may take three different orientations, thus, the red dot can be found in three different locations that are to be remembered. A block of trials started with a presentation of 1 pair of shapes and increases to the sequential presentation of 7 pairs of shapes. At the end of each block, the participant should recall the positions of the red dots by pointing at the picture with three possible locations marked exactly in the same order as the sets were presented. An example of the Spatial Recall subtest can be found at http://www.pearsonclinical.co.uk/ in a free demo version of the AWMA.
Working memory rating scale. The questionnaire includes 20 items which describe possible behavior manifestations of poor working memory in the classroom (e.g., “Puts hand up to answer a question but forgets what she/he intended to say”, “Requires regular repetition of instructions”). A teacher should identify how typical each behavior is for each particular child by rating them with one of the following responses: “not typical at all” (0 points), “occasionally” (1 point), “fairly typical” (2 points) or “very typical” (three points). Once all items have been completed, the sum of the raw scores can be calculated. Higher scores reflect greater deficits of working memory. The raw scores also can be converted to T scores with the help of the normative table provided in the WMRS Manual (Alloway, Gathercole, & Kirkwood, 2008).
Translation
Before test administration, both methods were translated into Russian by a linguist and a child neuropsychologist.
The materials from the Word Recall subtest were almost completely replaced by Russian one-syllable or disyllabic words (no longer than five letters, as some monosyllabic Russian words also contained five letters). The mean frequency of the 174 words was 145.426 ipm (instances per million words), Median = 35.450, IQR = 3726.4. The frequency of 66% of the words was between 5-100 ipm, the frequency of 29% of the words was higher than 100 ipm and only 5% fell below 5 ipm (Lyashevskaya & Sharov, 2009). Those words with a low ipm, for instance the Russian equivalent of the word cake ([keks], ipm =1.1) and rice ([ns], ipm = 4.8), were thoroughly analyzed and considered to be familiar and routine to every child.
The Listening Recall subtest was fully translated into Russian and only 7 out of a total of 174 sentences were changed in order to avoid ambiguity. In English, there is only one word form for adjectives and nouns (except the Genitive case), but Russian words vary according to their gender and case. Russian verbs are also conjugated for different nouns and pronouns. Therefore, a participant may need to remember both the last and antecedent words in order to recall the grammatical form correctly. This fact results in an additional memory load; moreover, children (especially young ones) who have not yet studied Russian grammar can have difficulty in understanding and following such a demand. Taking into account these specificities, the rules of the test were slightly transformed: we accepted as a correct recall any form of the last words (either the infinitive or conjugated form), thus ignoring the grammatical features which imposed an additional memory load.
Items for the Nonword Recall subtest were checked to ensure that they were nonwords.
Results
AWMA Results
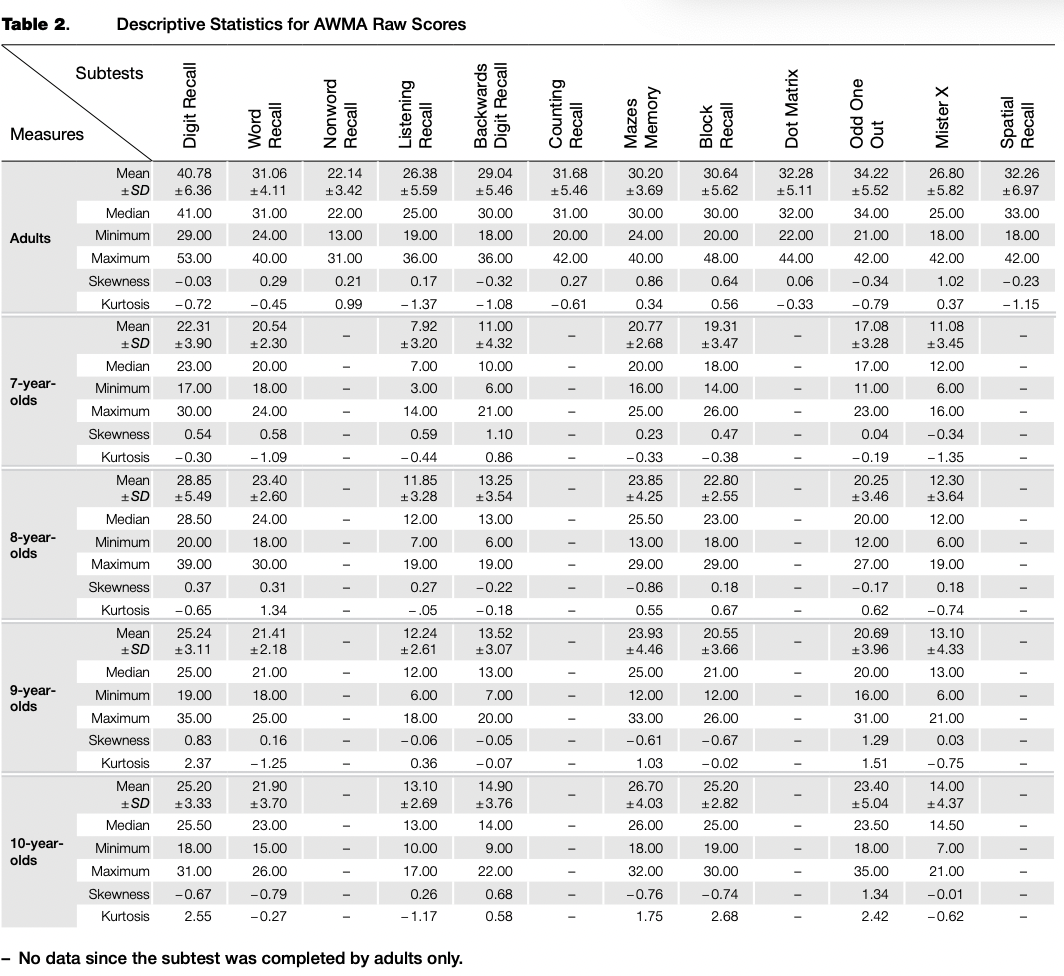
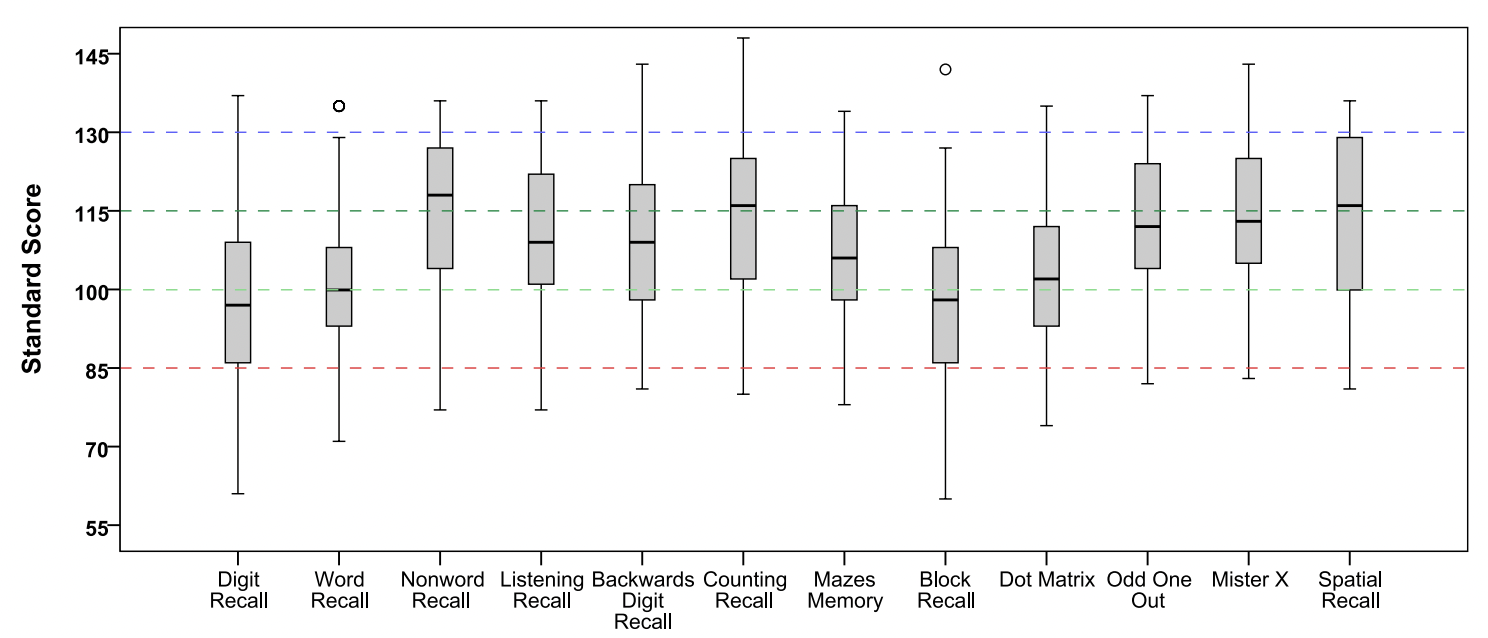
Descriptive statics for the raw scores of the AWMA subtests are provided in Table 2. The box-plots of standard scores are shown in Figure 2, and indicate that there were no lower outliers in any subtest (this allowed us to avoid the deletion of any participant’s data) and that the majority of results fell within average standard scores.
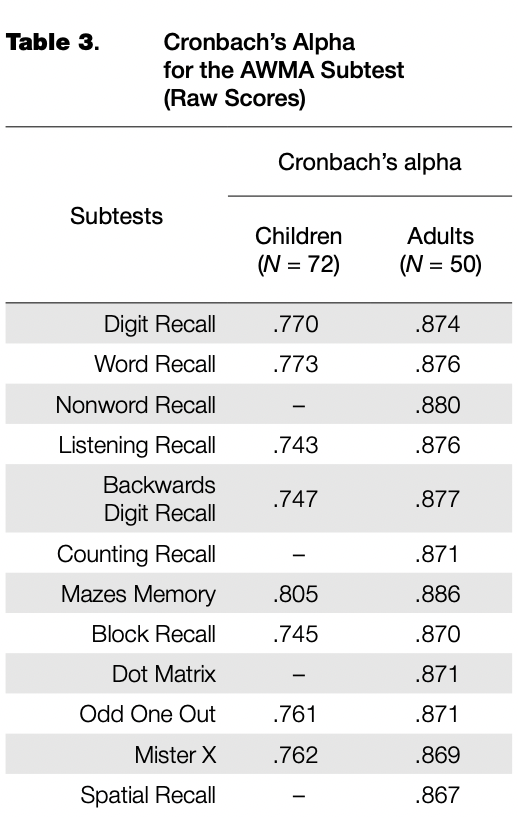
Estimates of Cronbach’s alpha were computed for each subtest in order to assess internal reliability (see Table 3). The analysis of internal reliability revealed acceptable values of alpha, ranging from .743 to .886.
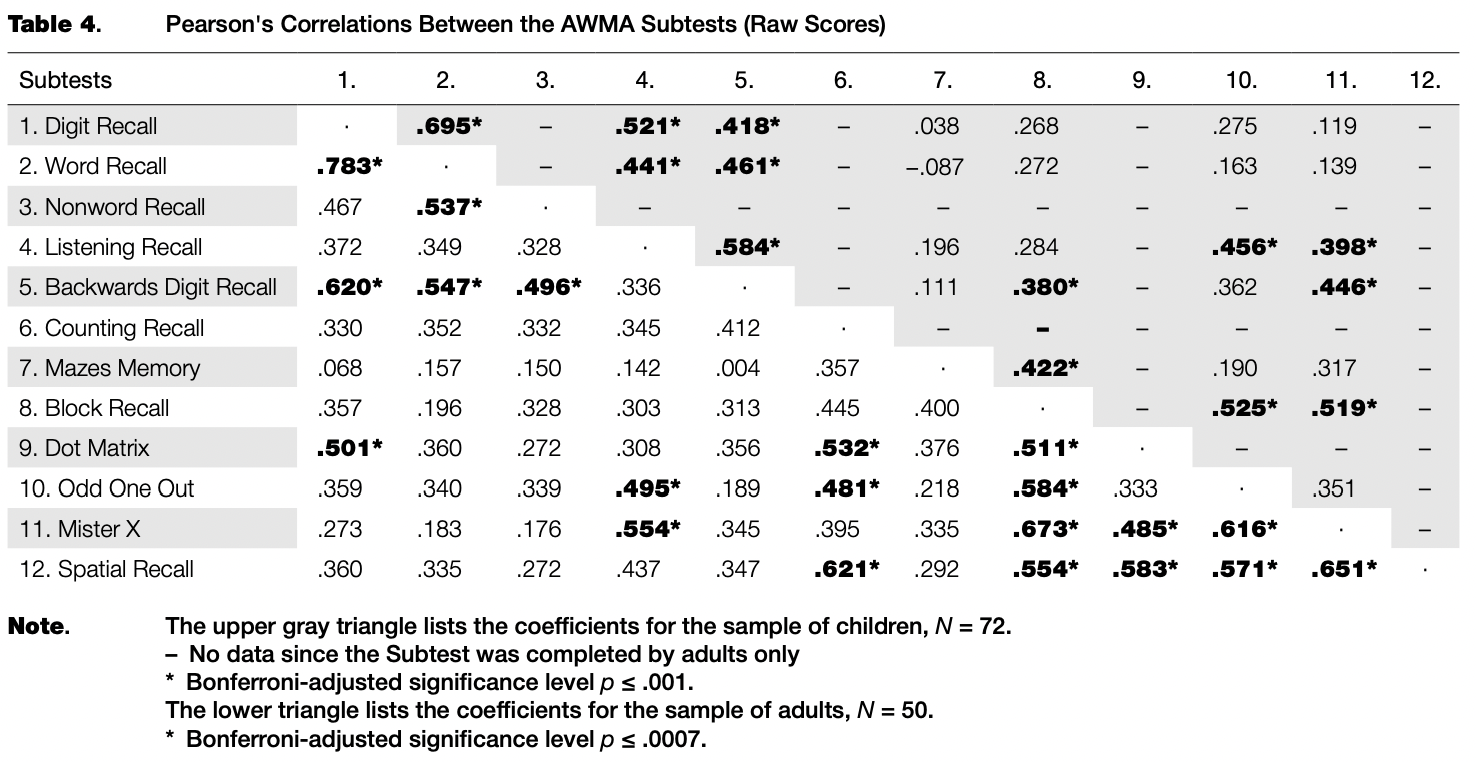
Table 4 lists Pearson’s correlations between all AWMA subtests. In the sample of children, the correlation analysis showed significant inter-correlations among all verbal subtests, which varied from .418 to .695; among all visuospatial subtests, which varied from .422 to .525; and among all working memory subtests, which varied from .398 to .456, with Bonferroni adjusted p < .001 in each case. In the sample of adults, the significant inter-correlations among all verbal subtests varied from .537 to .783; among all visuospatial subtests the variation was from .511 to .673; and among all working memory subtests the variation was from .481 to .621, with Bonferroni adjustedp < .0007 in each case.
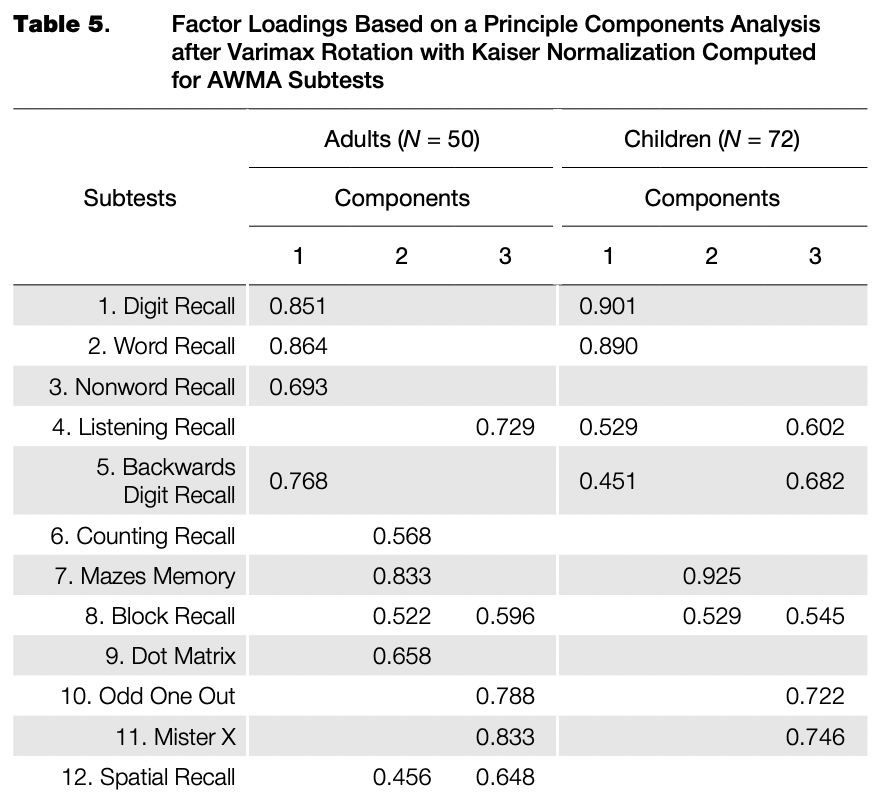
The principal components analysis revealed a three- factor structure accounting for about 70% of the total variance (see Table 5). An examination of the Kaiser- Meyer-Olkin measure of sampling adequacy suggested that the sample was factorable (in the sample of adults, KMO = 0.771; in the sample of children, KMO = 0.715) along with a significant departure from sphericity (in the sample of adults, x2 (66) = 297.374, p < .001; in the sample of children, x2 (28) = 202.773, p < .001). When loadings less than 0.40 were excluded, the analysis yielded a three- factor solution. In the sample of adults, Component 1 includes four verbal subtests; Component 2 includes four visuospatial subtests and the Counting Recall subtest which measures verbal WM and involves the processing of visuospatial information; Component 3 includes four WM subtest (both verbal and visuospatial) and the Block Recall subtest. In the sample of children, Component 1 includes all the verbal subtests completed by children; Component 2 includes two visuospatial subtests; Component 3 includes all the WM subtests completed by children (both verbal and visuospatial) and the Block Recall subtest.
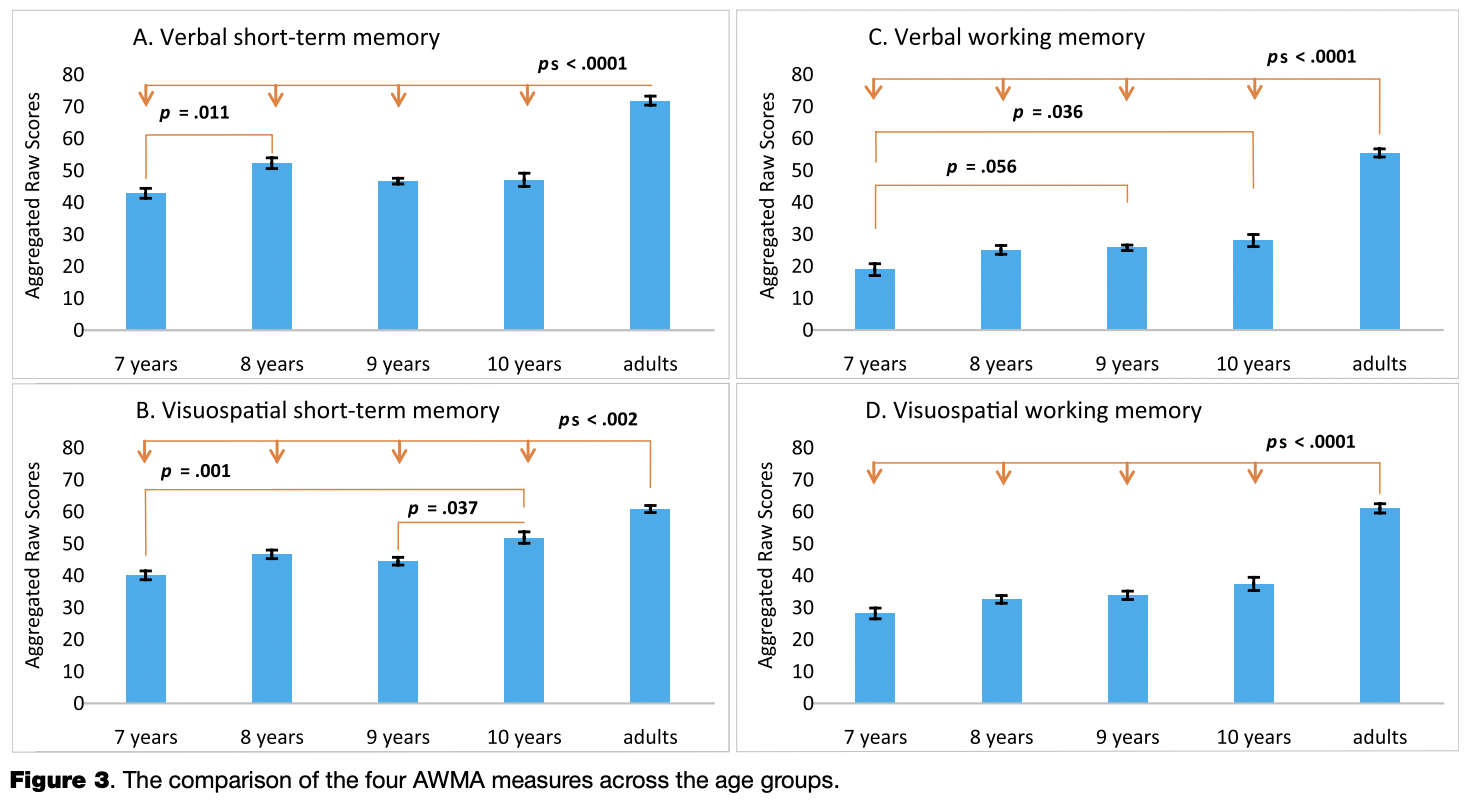
Despite the fact that this study included a relatively small sample of children, an analysis of age-dependent differences was also conducted in order to show a perspective of research application and somehow validate the current study in the scope of the declared age-sensitivity of AWMA measures. A one-way ANOVA was used to compare all four memory components (verbal short-term memory, verbal working memory, visuospatial short-term memory and visuospatial working memory) across the age groups. An analysis was conducted separately for each memory component, due to the fact that each AWMA subtest has its own score maximum. Hence, the dependent variables were the sum of the raw scores of each two corresponding subtests: verbal short-term memory included the results of Digit Recall and Word Recall; verbal working memory included Listening Recall and Backwards Digit Recall; visuospatial short-term memory included Mazes Memory and Block Recall; visuospatial working memory included Odd One Out and Mister X. The following main effects of Age Ggoup were observed for all memory components: verbal short-term memory (F(4,117) = 72.595, p < .0001, q2p = .713), verbal working memory (F(4,117) = 135.203, p < .0001, q2p = .822), visuospatial short-term memory (F(4,117) = 42.687, p < .0001, q2p = .593) and visuospatial working memory (F(4,117) = 88.957, p < .0001, i)2p = .753), as indexed by Wilks’ Lambda criterion. Post-hoc pairwise comparisons were conducted with Bonferroni adjustment; see Figure 3 with plotted significant p-values.
Academic Performance and Working Memory
Due to the fact that AWMA is considered as a predictive measure of academic performance, we collected the final year scores gained by the children in five main courses: Writing, Reading, Foreign Language, Mathematics and Science (introductory academic science course titled “Okru- zhayuschiy mir” [“The world around us”]). Russian schools use a five-point academic grading system. From the beginning of the second year, children are rated for quizzes, tests, reports and many different written and oral tasks during each quarter of an academic year. At the end of each quarter and then at the end of the year they get a final credit that is the summary of the final quiz and the history of ratings throughout the academic year. Figure 4 provides the distribution of the final year scores earned by 57 children aged 8-10 (the 2nd and the 3rd year).
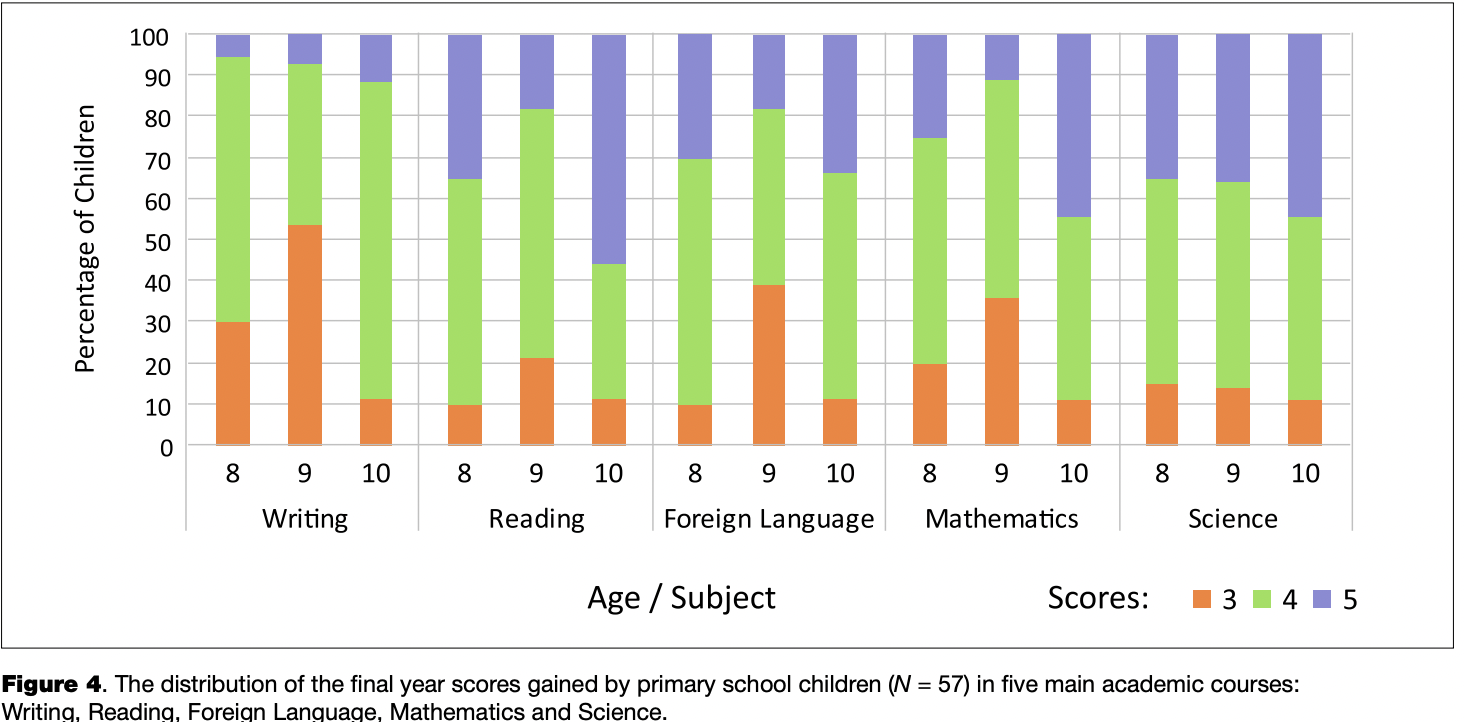
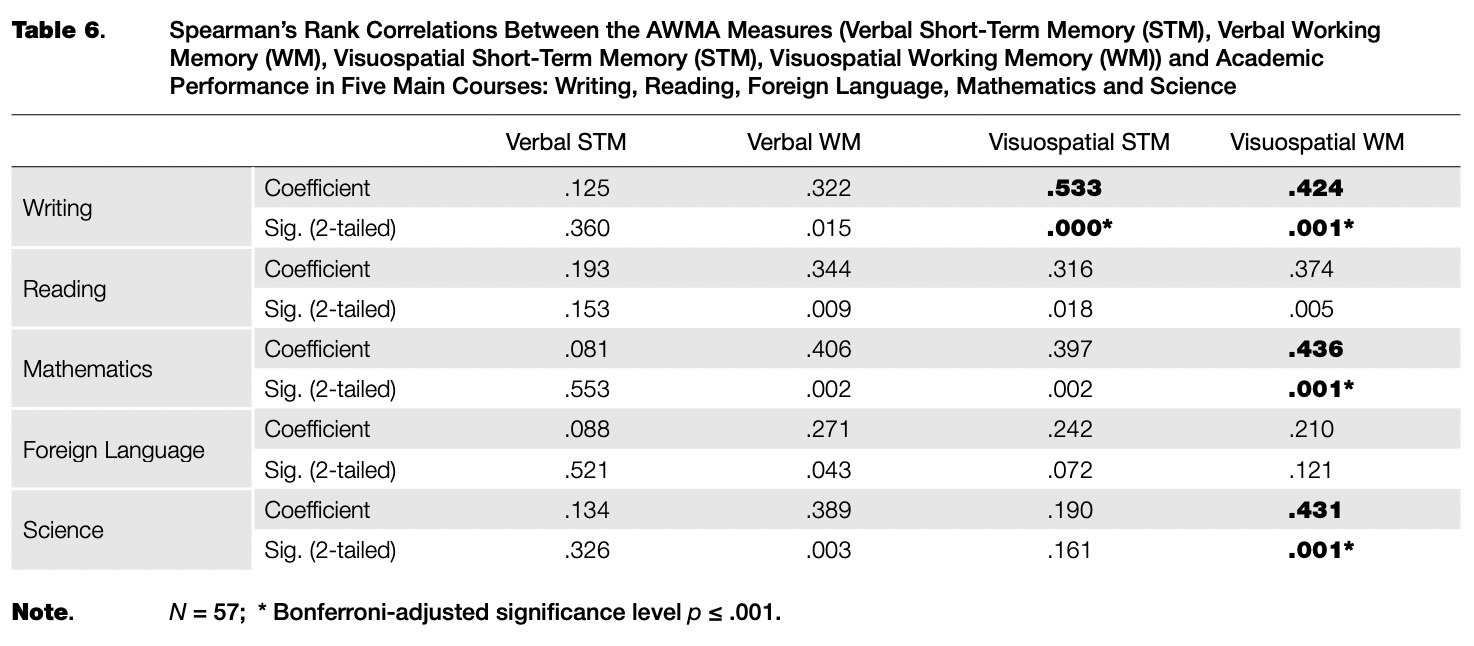
Table 6 lists Spearman’s rank correlations between the AWMA measures and academic performance in five main courses: Writing, Reading, Foreign Language, Mathematics and Science (Figure 4). The significant correlations indicate that Writing, Mathematics and Science are associated with visuospatial WM ability and, along with WM, visuospatial STM is also linked to academic achievement in Writing.
WMRS Results
The WMRS scores were collected for 69 children, with a mean of 15.67 points ± 14.09, varied from 0 to 46 points, and were positively skewed (skewness = 0.871). Further analysis showed a high value of WMRS internal consistency (Cronbach’s alpha = .970). Pearson’s correlation analysis revealed a statistically significant inter-correlation of WMRS scores and verbal WM measured by the AWMA subtests (.331 with Bonferroni-adjusted, p = .025). The other AWMA measures did not show any significant correlations with WMRS ratings. Moreover, the WMRS scores significantly correlated with academic performance in all of the main courses (N = 57): Writing (-.600), Reading (-.581), Mathematics (-.535), Foreign Language (-.612) and Science (-.410), with Bonferroni- adjusted p’s < .003.
Case Study 1
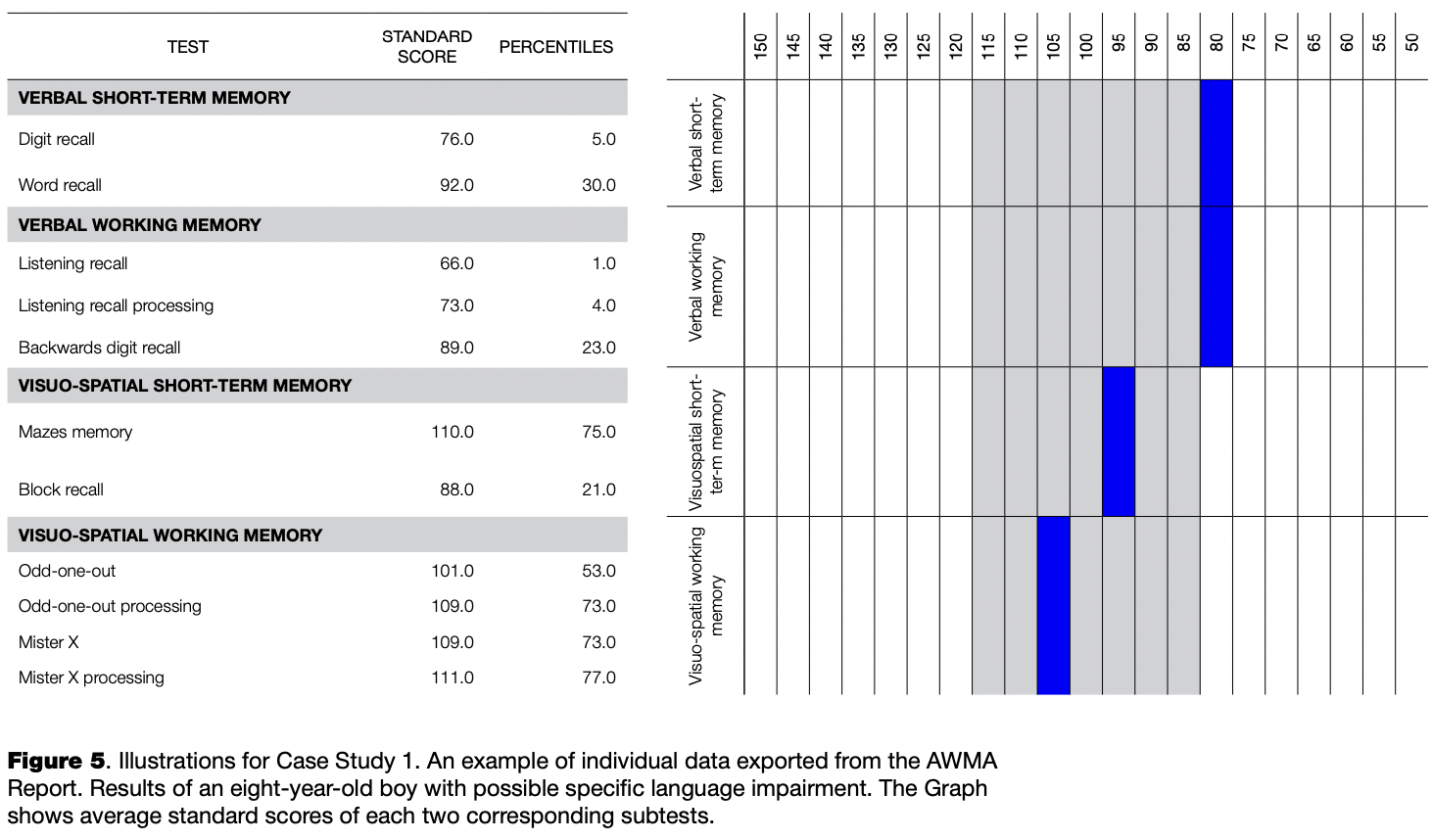
Case Study 1 follows an eight-year-old boy (age at testing: 8 years and 8 months, class: the second grade) with severe learning difficulties in acquiring reading, writing, mathematics, foreign language and science at a regular Moscow school. The boy was previously diagnosed as having intellectual development disorder. During the electrophysiological examination, local EEG deviant patterns were observed over his left temporal brain area, which are typical for children with verbal deficits. At the time of testing, the boy’s academic performance was the poorest in his class. During the lessons he struggled to follow instructions and used to give an answer of “no” when he was asked to repeat a task. He was also usually frustrated when trying to copy any verbal material, especially when it was dictated orally by the teacher. His teacher believes that the boy is sometimes unable to understand speech. In the WMRS questionnaire, he was rated with 41 points and identified as being at risk of poor educational progress over the coming years. His AWMA scores are shown in Figure 5.
Interpretation
The boy’s memory profile appeared to be similar to those of children with specific language impairment (SLI), as reported in (Archibald & Gathercole, 2006; Alloway, Rajendran, & Archibald, 2009; Alloway & Stein, 2014). The fact that both visuospatial scores fell within the standard scores range of 95-105 showed that the boy was able to complete tasks with visual support and could manipulate visuospatial information. This completely agrees with the data in (Archibald & Gathercole, 2006), a study which tested children with SLI and found that along with deficits in verbal WM and STM these children performed at agelevel on visuospatial WM measures; however, according to the findings, poor verbal storage is expected to have a detrimental impact on learning. It is believed that these results and their interpretation can contribute to the development of the support-learning program for the boy.
Case Study 2
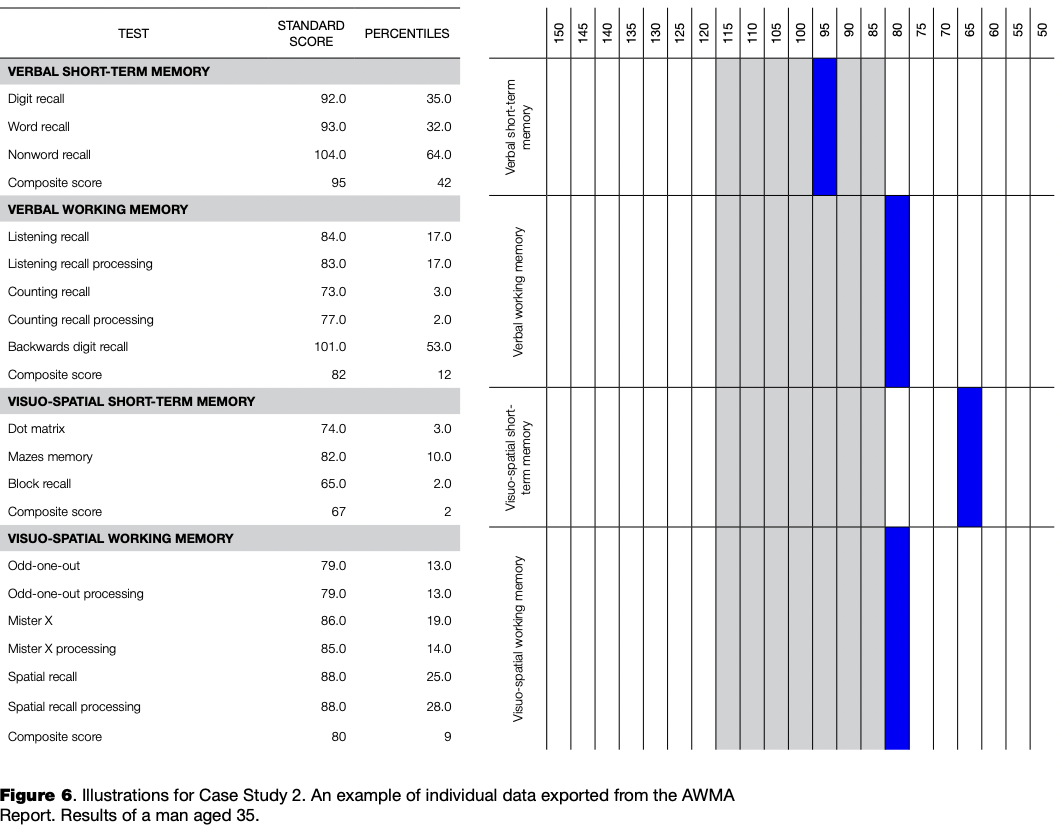
Case Study 2 follows a 35-year-old man who works in the field of marketing and complained about severe memory difficulties which seemed to be getting worse over the last few years. However, he had never been diagnosed with any impairment. The man has difficulties in remembering almost all types of information and can not imagine his life without memory aids. When talking to his friends he can sometimes lose the information he heard several minutes earlier and cannot always remember what he was going to say. He characterizes himself as an inattentive person and not as successful as he wants to be. His grandmother was diagnosed with Alzheimer disease. The man’s AWMA scores are shown in Figure 6.
Interpretation
The memory profile shows pronounced memory difficulties, and especially poor performance on the visuospa- tial measures. His visuospatial memory span approaches the that of children aged 7-8. This pattern of results may point to some neurological condition, including the early stages of Alzheimer disease which is characterized by a deficit in memory as the most remarkable feature. It has been reported that some of the earliest signs of preclinical disease may occur in tests of visuospatial skills (e.g., Johnson, Storandt, Morris, & Galvin, 2009; Camacho-Valadez, 2015). Unfortunately, most cases of Alzheimer disease are caused by gene mutations that can be passed from parent to child (e.g., Horgusluoglu, Nho, Risacher, & Saykin, 2015). This fact implies a risk of poor genetics. The man was recommended to undergo a detailed medical examination and consultation.
Discussion
During the administration of the AWMA, it was confirmed that all translated and recorded instructions were well understood. Despite of the fact that the distribution of scores in some subtests departs from the normal curve, the internal reliability analysis showed acceptable values indicating a normal level of internal reliability of the AWMA measures.
The results of the between-subtests correlation analysis are consistent with Baddeley”s model of working memory: significant correlations were observed among the subtests aimed at measuring (1) active and passive verbal storage (Digit Recall, Word Recall, Nonword Recall, Listening Recall, Backward Digit Recall, Counting Recall), (2) active and passive visuospatial storage (Mazes Memory, Block Recall, Dot Matrix, Odd One Out, Mr. X, Spatial Recall) and (3) executive capacity to maintain both verbal and visuospatial information in WM (Listening Recall, Backward Digit Recall, Counting Recall, Odd One Out, Mr. X, Spatial Recall). These results were also supported by the principle component analysis, which revealed a three-component empirical structure consistent with the previously reported data (e.g, Nadler & Archibald, 2014). The departure of the present PC A results from those reported in the Nadler & Archibald (2014) study may well be due to statistical fluctuations caused by our relatively limited sample.
However, it should be mentioned here that the PCA is not very telling with regard to the latent structure of this particular data. This is because the authors of the original study (Alloway, Gathercole, & Pickering, 2006), when analyzing the normative AWMA sample, applied a confirmatory factor analysis to choose among several competing theoretically-driven models. Our analysis revealed that the best fitting model includes three factors which are not mutually orthogonal but show a great deal of correlation. These three nonorthogonal factors correspond to three components of the Baddeley and Hitch (1974) WM model, with the executive component being supported by a common resource pool and two passive domain-specific storages. It is clear that orthogonal principal components are unable to represent such a hierarchical structure. Nonetheless, the fact that the PCA resulted in three components indirectly supports the notion that latent space dimensionality equals three.
The age-related analysis revealed that not all AWMA measures demonstrated significant developmental increases in children from 7 to 10 years of age, possibly due to the fact that the study was limited by the small sample size. However, the results reflect consistency with age-related improvements in STM and WM reported in previous studies (e.g., Alloway & Alloway, 2013).
Among the correlations computed between the AWMA and WMRS scores, the significance level was reached only between the WMRS and AWMA verbal working memory measure. This is consistent with the data reported in a previous study (Politimou, Masoura, & Kiosseoglou, 2015). Politimou and colleagues observed a strong relationship between the Greek version of WMRS and children’s verbal ability (vocabulary knowledge), and suggested that verbal skills might imply a sort of bias in teachers’ behavioral ratings.
Regarding the correlations of the AWMA measures and academic performance, it should be noted that Russian grading is a rather subjective system. Even though it varies from 1 to 5 points, “1” is seldom used; scores of 1 or 2 points are almost never used for the final credits. If one’s academic performance is worth 2 points at the end of the year, the child has to repeat the course or change schools. Furthermore, a child who scores 3 points can sometimes approach 4 points or can be struggling to get those 3 points. However, the results of Spearman’s correlation analysis indicate relatively weak but reasonable links between some AWMA measures and learning outcomes. For instance, Writing appeared to be associated with visuospatial STM and WM, which is consistent with the demands placed upon the remembering of letter images, their visuospatial orientation, cursive variants, etc. during handwriting.
It should also be noted that the translated AWMA seems to be sensitive to the WM deficits in atypical populations (Case Studies 1 and 2), although this is a topic for further investigation.
In conclusion, the results of the two methods’ application suggest that the variants translated into Russian are suitable for further usage, but they require expanded adaptation and elaboration for larger Russian samples.
References
Alloway, T.P. (2007). Automated Working Memory Assessment: Manual. London: Pearson Assessment.
Alloway, T.P. (2009). Working memory, but not IQ, predicts subsequent learning in children with learning difficulties. European Journal of Psychological Assessment, 25(2), 92-98. doi: 10.1027/1015-5759.25.2.92
Alloway, T.P. (2011). A comparison of working memory profiles in children with ADHD and DCD. Child Neuropsychology, 17(5). 483-494. doi:10.1080/09297049.2011.553590
Alloway, T.P. (2012). The neurophysiological performance of visuospatial working memory in children with developmental coordination disorder. Developmental Medicine & Child Neurology, 54(12), 1075-1076. doi: 10.1111/i. 1469-8749.2012.04427 X
Alloway, T.P., & Alloway, R.G. (2010). Investigating the predictive roles of working memory and IQ in academic attainment. Journal of Experimental Child Psychology, 106(1), 20-29. doi:10.1016/i.iecp.2009.11.003
Alloway, T.P., & Alloway, R.G. (2013). Working memory across the lifespan: A cross-sectional approach. Journal of Cognitive Psychology, 25(1), 84-93. doi:10.1080/204459U.2012.7 48027
Alloway, T.P., Alloway, R.G., & Wootan, S. (2014). Home sweet home: Does where you live matter to working memory and other cognitive skills? Journal ofExperimental Child Psychology, 124(August), 124-131. doi: 10.1016/j.jecp.2013.11.012
Alloway, T.P., & Copello, E. (2013). Working memory: The what, the why, and the how. The Australian Educational and Developmental Psychologist, 30(02), 105-118. doi:10.1017/ edp.2013.13
Alloway, T.P., Gathercole, S.E., & Kirkwood, H. (2008). Working Memory Rating Scale (WMRS): Manual. London: Pearson Assessment.
Alloway, T.P., Gathercole, S.E., Kirkwood, H., & Elliott, J. (2008). Evaluating the validity of the automated working memory assessment. Educational Psychology, 28(7), 725-734. doi: 10.1080/01443410802243828
Alloway, T.P., Gathercole, S.E., Kirkwood, H., & Elliott, J. (2009). The working memory rating scale: A classroombased behavioral assessment of working memory. Learning and Individual Differences, 19(2), 242-245. doi:10.1016/i. lindif.2008.10.003
Alloway, T.P., Gathercole, S.E., & Pickering, S.J. (2006). Verbal and visuospatial short-term and working memory in children: Are they separable? Child Development, 77(6), 1698-1716. doi: 10.1111/j. 1467-8624.2006.00968.X
Alloway, T.P., Rajendran, G., & Archibald, L.M.D. (2009). Working memory in children with developmental disorders. Journal of Learning Disabilities, 42(4), 372-382. doi: 10.1177/0022219409335214
Alloway, T.P., & Stein, A. (2014). Investigating the link between cognitive skills and learning in non-comorbid samples of ADHD and SLI. International Journal of Educational Research, 64, 26-31. doi:10.1016/j.ijer.2013.10.003
Alloway, T.P., & Temple, K.J. (2007). A comparison of working memory skills and learning in children with developmental coordination disorder and moderate learning difficulties. Applied Cognitive Psychology, 21(4), 473-487. doi:10.1002/ acp.1284
Alloway, T.P., Wootan, S., & Deane, P. (2014). Investigating working memory and sustained attention in dyslexic adults. International Journal of Educational Research, 67, 11-17. doi:10.1016/j.ijer.2014.04.001
Archibald, L.M.D., & Gathercole, S.E. (2006). Short-term and working memory in specific language impairment. International Journal of Language & Communication Disorders, 41(6), 675-693. doi:10.1080/13682820500442602
Baddeley, A. (1992). Working memory. Science, 255(5044), 556-559. doi:10.1126/science, 1736359
Baddeley, A. (2010). Working memory. Current Biology, 20(4), R136 - R140. doi: 10.1016/j.cub.2009.12,014
Baddeley, A.D., & Hitch, G. (1974). Working memory. In G. Bower (Ed.), Psychology of learning and motivation, Vol. 8. (pp. 47-89). New York: Academic Press.
Bayliss, D.M., Jarrold, C., Gunn, D.M., & Baddeley, A.D. (2003). The complexities of complex span: explaining individual differences in working memory in children and adults. Journal of Experimental Psychology: General, 132(1), 71-92. doi:10.1037/0096-3445.132,l,7
Camacho-Valadez, D. (2015). Time perception and visual working memory in Alzheimer disease. Paper presented at the Second Border Biomedical Research Center Symposium, University of Texas at El Paso.
Chrysochoou, E., Masoura, E., & Alloway, T.P. (2013). Intelligence and working memory: Contributions to reading fluency, writing and reading comprehension in middle school-age children. In V. Deliyanni, А. Вака, E. Figou, & D. Moraitou (Eds.), Scientific annals — School of Psychology A.U.Th, Vol. X. (pp. 226-251). Thessaloniki: Office of Aristotle University Publications.
Engel de Abreu, P.M.J., Nikaedo, C., Abreu, N., Tourinho, C.J., Miranda, M.C., Bueno, O.F.A., & Martin, R. (2014). Working memory screening, school context, and socioeconomic status: An analysis of the effectiveness of the Working Memory Rating Scale in Brazil. Journal of Attention Disorders, 18(4), 346-356. doi:10.1177/1087054713476138
Engel de Abreu, P.M.J., Santos, F.H., & Gathercole, S.E. (2008). Are working memory measures free of socioeconomic influence? Journal of Speech, Language, and Hearing Research, 51(6), 1580-1587. doi:10.1044/1092-4388(2008/07-0210
Gathercole, S.E., Alloway, T.P., Willis, C., & Adams, A.-M. (2006). Working memory in children with reading disabilities. Journal of Experimental Child Psychology, 93(3), 265-281. dQi;10.l016/j.jecp,2005.08,003
Gathercole, S.E., Lamont, E., & Alloway, T.P. (2006). Working memory in the classroom. In S.J. Pickering (Ed.), Working memory and education (pp. 219-240). Amsterdam, Boston, Mass.: Academic Press.
Holmes, J., Hilton, K.A., Place, M., Alloway, T.P., Elliott, J.G., & Gathercole, S.E. (2014). Children with low working memory and children with ADHD: same or different? Frontiers in Human Neuroscience, 8, 976:1-13. doi: 10.3389/ fnhum.2014.00976
Horgusluoglu, E., Nho, K., Risacher, S.L., & Saykin, A.J. (2015). Pathway-based gene analysis identifies VEGFA as a gene associated with cerebral blood flow in Alzheimer's disease. Alzheimer's & Dementia: The Journal of the Alzheimer's Association, 11(7), P855. doi:10.1016/i.ialz.2015.08.023
Injoque-Ricle, I., Calero, A.D., Alloway, T.P., & Burin, D.I. (2011). Assessing working memory in Spanish-speaking children: Automated Working Memory Assessment battery adaptation. Learning and Individual Differences, 21(1), 78-84. doi:10.1016/j.lindif.2010.09.012
Johnson, D.K., Storandt, M., Morris, J.C., & Galvin, J.E. (2009). Longitudinal study of the transition from healthy aging to Alzheimer disease. Archives of Neurology, 66(10), 1254-1259. doi:10.1001/archneurol.2009.158
Lyashevskaya, O.N., & Sharov, S.A. (2009). [Frequency dictionary of the modern Russian language (the Russian National Corpus)]. Moscow: Azbukovnik. (In Russian).
Nadler, R., & Archibald, L. (2014). The assessment of verbal and visuospatial working memory with school age Canadian children. Canadian Journal of Speech-Language Pathology and Audiology, 33(3), 262-279.
Normand, S., & Tannock, R. (2014). Screening for working memory deficits in the classroom: The psychometric properties of the working memory rating scale in a longitudinal schoolbased study. Journal of Attention Disorders, 18(4), 294-304. ІОІШШ22/1Л820542124450^
Politimou, N., Masoura, E., & Kiosseoglou, G. (2015). Working Memory Rating Scale's utility to identify children's memory difficulties in diverse educational environments: Can it work in every school? Applied Cognitive Psychology, 29(2), 291-298. doi:10.1002/acp.3107
Wechsler, D. (2003). Wechsler intelligence scale for children- Fourth Edition (WISC-TV). San Antonio, TX: The Psychological Corporation.
Related Articles
Sergei Yu. Korovkin
Ilya Yu. Vladimirov
Anna D. Savinova
Koshkin Roman
Ossadtchi Alex
Shtyrov Yury